While chest tube placement (tube thoracostomy) is one of the more simple and straight-forward procedures in thoracic surgery, chest tube management can be fraught with frustration for both patients and providers. While the system itself is relatively uncomplicated, it is area that often brings stress to nurses and other axillary providers who do not work with chest tubes on a daily basis.

Ambulating with chest tubes is an exercise in logistics
Chest tubes can be knocked over, dislodged or accidentally removed from suction before the lung is completely healed. Chest tubes also make any sort of ambulation just a little bit more complex. The logistics of ambulating patients with one (or more pleurovacs) in addition to IV pumps, poles, foley catheters and other devices, particularly if the patient is weak or unsteady more of a chore than many can image. A ten minute walk make take upwards of fifteen minutes in preparation, as supplies are gathered and additional personnel are summoned for assistance.
Is there an air leak?
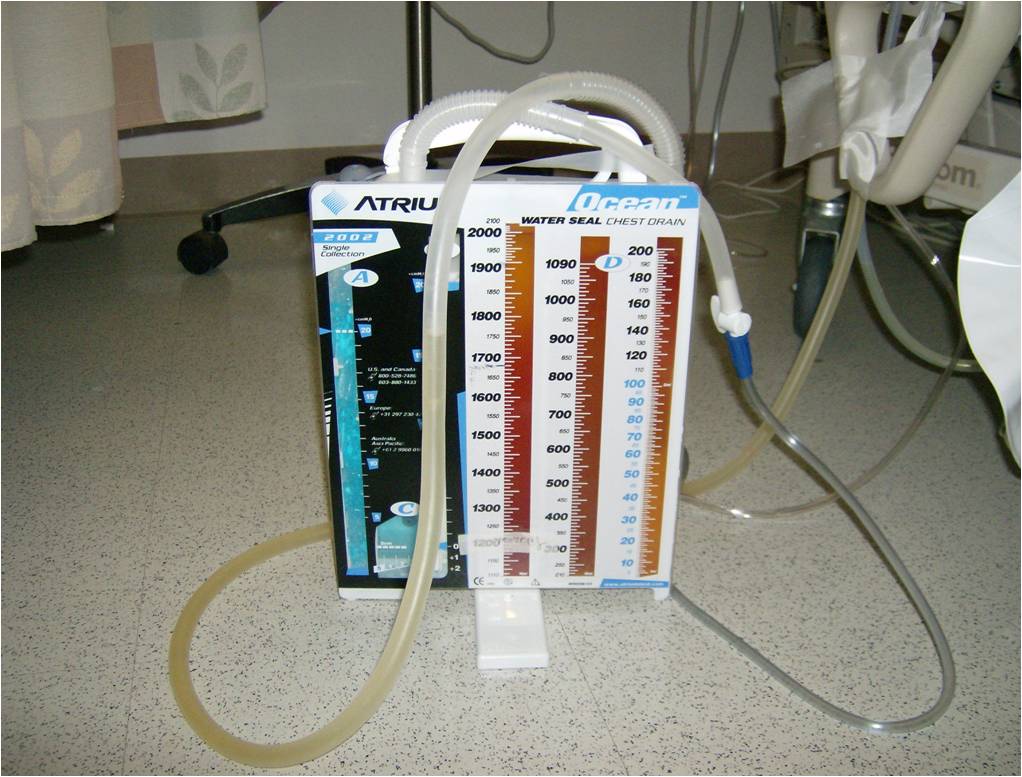
But this is only one of the frustrations of chest tube management. The main point of contention and frustration for providers and patients alike is monitoring chest tubes for the presence / absence of an air leak, and calculating drainage. While neither of these tasks is particularly arduous, accuracy is critically important. Both the miscalculation of drainage as well as the report of a newly developed air leak (or an previously undetected but continued air leak) can cause significant delays in chest tube removal. Or, if the chest tube is removed too early, it can cause a pneumothorax or re-accumulation of a pleural effusion.

The first problem can be readily addressed with use of an orange (or other non-standard color) sharpie marker. The second problem can require a bit of ingenuity, especially since the development or detection of an air leak can occur during the course of the day -after the thoracic surgery team has been in to evaluate the patient (for example). In fact, it’s one of the frequent calls we field on a daily basis.
Nurse: Ummm.. did this patient have an air leak this morning? (Or with more experienced nurses): “Mr. X developed a small air leak about an hour ago after walking in the hall.”
Then the question becomes one of whether or not the chest tube (which may have been previously scheduled for removal) can be removed. Often, it delays chest tube removal by another day to ensure that the lung is adequately healed.

Why can’t I just cross my fingers and pull it anyway?
Or we can proceed at our own peril – and risk taking out the chest tube. Sometimes the lung stays up, but often – the patients develop a pneumothorax, requiring another chest tube to be placed. Replacing the chest tube is not just an otherwise unnecessary procedure (and all the risks entailed), it’s painful for the patients, as well as being very demoralizing for the patient.
Several thoracic surgeons have attempted to solve this problem using a myriad of devices – from portable suction machines to more novel ideas like computerized chest tube systems such as the device developed by Dr. Gaetano Rocco. Dr. Rocco’s device was a computer that allowed patients with prolonged air leaks to be discharged home with real-time monitoring. (It was essentially a laptop computer, and requires use of a specialized chest tube system). It’s still a great development, but fairly expensive for use in hospitalized patients.
Additionally and unfortunately, most of these devices have failed to gain mainstream attention, or use – which means that despite all of the new technologies and techniques, many of our patients are still chained to their rooms (to the suction module) while waiting for their lung to heal. This puts the patients at risk for additional complications in addition to prolonging their hospital stay.
Now Dr. Chin-Hao Chen et al. have designed a new device that can be used with the existing pleurovac systems to perform real-time pressure monitoring. The paper, published in a recent issue of the Journal of Thoracic Disease demonstrates how surgeons can add this device to existing closed systems to detect air leaks and chest tube tidaling. This type of device allows surgeons to adopt state-of-the-art technologies using the standard equipment already available in their hospitals with minimal modifications. It eliminates the question of when the is lung healed, and when can the chest tube be removed.
References and additional reading
Article cited above:
Chin-Hao Chen, Tsang-Pai Liu3,4, Ho Chang5, Tung-Sung Huang3,4, Hung-Chang Liu1,2,3, Chao-Hung Chen (2015). A chest drainage system with a real-time pressure monitoring device. Journal of Thoracic Disease, (July 2015) 7:7.
Chest Tube Management (2007) Powerpoint from a presentation at DRMC in Danville, Virginia.
Kwiatt M1, Tarbox A2, Seamon MJ3, Swaroop M4, Cipolla J5, Allen C6, Hallenbeck S6, Davido HT7, Lindsey DE8, Doraiswamy VA9, Galwankar S10, Tulman D11, Latchana N11, Papadimos TJ8, Cook CH8, Stawicki SP8. (2014). Thoracostomy tubes: A comprehensive review of complications and related topics. Int J Crit Illn Inj Sci. 2014 Apr;4(2):143-55. doi: 10.4103/2229-5151.134182.
