It’s not too late to register for the upcoming Thoracic Oncology Symposium in Catania, Italy. The symposium is being held April 6th and 7th and is sponsored by the University of Catania and Policlinico University Hospital.
This year’s topic is “Surgery for “advanced” lung and esophageal cancer: New horizons or a false dawn?” Lectures include a presentation by Dr. Migliore on HITHOC for M1 lung cancer, a discussion on the use of hyperthermia, as well as several lectures on the use of VATS in advanced lung cancer and a segment devoted to esophageal cancer that includes the presentation of research findings by Dr. Toni Lerut based on findings from 3000 esophagectomies.
The full program and registration information can be seen Here. Potential registrants may also contact Dr. Migliore at mmiglior@unict.it
A guest post on last year’s conference is viewable here.
Talking to Dr. Benny Weksler about Minimally invasive esophagectomies, robotic surgery, lung cancer screening and life in the mid-south.
Memphis, Tennessee USA
Recently, I had the great pleasure and privilege to have a sit down interview with one of the thoracic surgeons whose work I have long admired. Loyal readers will certainly recognize the name, Dr. Benny Weksler, one of the modern masters of esophageal surgery.
Minimally invasive esophagectomies (MIE)
He is best known for his minimally invasive esophagectomies which take much of the pain (literally) out of the traditional surgical resection for esophageal cancer. The minimally invasive esophagectomy is the VATS approach to esophagectomy, using smaller 2 to 3cm ‘ports’ instead of large incisions.
In classic thoracic surgery, large open incisions such as the Ivor Lewis esophagectomy were the best way to optimize survival for patients with this aggressive cancer. However, the traditional open surgery itself is particularly arduous and has been likened to the “open heart surgery” of the thoracic specialty. The Ivor Lewis in particular is two full-sized surgeries; a full thoracotomy combined with a transverse laparotomy. While it has been utilized for decades for excellent visualization, staging and resection, the recovery is a long, painful process.
Dr. Weksler in the mid-south
It’s been just over three years since Dr. Benny Weksler was recruited to start a new thoracic surgery program at The University of Tennessee – West Cancer Clinic – Methodist Hospital System here in Memphis, Tennessee. It’s been a big change, and a bit of an eye-opening experience for the Brazilian native and famed thoracic surgeon who has spent much of this career in the northeast. Prior to this, he was part of the renowned University of Pittsburgh Medical Center under the famed Dr. James Luketich. Since Dr. Weksler’s move, he’s still adjusting to the warmer weather here, which is one of the things he likes best about the area along with the traditional Memphis music scene, which the city is famous for.
Memphis is more than just the home of Elvis Presley
It’s also been a time of great changes and innovations for Memphis and the University of Tennessee, as well. Dr. Weksler started the first thoracic surgery service line for the UT – Methodist Hospital system, which is actually the first real dedicated thoracic surgery service line in the Memphis area – which extends across a tri-state area that also covers parts of northern Mississippi and western Arkansas.
Memphis, Tennessee at night
Why is this important and what does it mean for Memphis?
Prior to Dr. Weksler’s arrival, patients were either referred to private cardiothoracic surgery practices in Memphis, they went to larger cities with bigger academic centers or they unwittingly trusted their health to a non-specialty surgeon. Neither of those options were ideal, but now patients in the northern Mississippi delta – metro Memphis area can receive state-of-the-art, surgical excellence close to home. For some patients, this is a matter of life or death.
Now the program is growing; so much so, that Dr. Weksler has two full-time thoracic surgeons and is actively looking for a third. With the addition of the third surgeon, Dr. Weksler hopes to expand the UT program to serve local veterans at the Memphis VA.
University of Tennessee affiliated – Methodist Hospital (official UT photo)
While Dr. Weksler doesn’t embrace the principles of uniportal surgery, his work on esophagectomies more than makes up for it. In fact, Dr. Weksler is one of the leading surgeons in the United States for minimally invasive esophagectomies. As discussed in previous posts, an experienced esophageal surgeon is critical for patient survival. (Bare Minimum competency for any esophageal surgeon is 25 cases a year – it’s not a surgery for your ‘average’ thoracic surgeon or any general surgeon).
Memphis’ newest secret weapon against cancer (too bad no one knows that he’s here)
In fact, his presence here in Memphis, among otherwise limited surgical services, is like finding a diamond while scavenging for supper in a metal dumpster in a hundred degree heat. In addition to being one of the foremost surgeons for esophageal disease (cancer and benign esophageal disease like achalasia), Dr. Weksler is also an experienced robotic surgeon.
As a newcomer to town, Dr. Weksler is having to re-build his practice volumes. As he explains, “We do about 30 esophagectomies a year, and I also see approximately 60 patients with esophageal cancer that cannot be operated on. 100% of our esophagectomies since I have been here were done minimally invasive”.
I can only speculate as a knowledgeable outsider that these surgical volumes reflect the lack of the general public and referring physicians knowledge about Dr. Weksler’s presence in the mid-south. Dr. Weksler is the type of surgeon that patients will travel across the country to see. My guess is that many of these potential patients are still traveling to Pittsburgh.
New ideas, new programs and new service lines
Dr. Weksler brings with him new ideas and new programs aimed at treating all Memphians. This includes community programs aimed at underserved and at-risk communities. One of these programs focuses on the diagnosis and treatment of lung cancer in African -American communities, which are disproportionately affected by advanced lung cancer, particularly in middle-aged males. By creating and implementing screening programs in these communities, Dr Weksler and his team are able to diagnose and treat lung cancers at earlier stages and improve patient survival. Despite being in its infancy, the program (which does not have a formal name) has screened over 100 patients and diagnosed eight cancers.
If you are a Memphis resident and would like information on this screening program or lung cancer screening: Contact the Lung Cancer Screening Navigator at Dr. Weksler’s office at 901-448- 2918.
Changing the art of Medicine & Surgery in Memphis
Dr. Weksler has been instrumental in creating at atmosphere of multidisciplinary collaboration. For example, programs have been streamlined and designed with patients in mind, to be the most effective, informative and efficient. This means that patients receive a “one stop shopping” experience as Dr. Weksler describes it. Patients are able to see their medical oncologist, thoracic surgeon and radiation oncologist on the same visit. All patients and their cases are presented at tumor board, to determine that treatment is individualized to the patient’s condition, functional status and tumor type which adhering to the clinical guidelines and evidence-based practice to optimize patient outcomes and long-term survival.
Q & A with Dr. Weksler – What patients should expect
Dr. Weksler talked to me at length about this multidisciplinary team approach as well as what patients should expect when they come to Methodist/ West Cancer center for care.
Question: What is the general process/ timeline for patient who has been referred to your clinic for evaluation?
Dr. Weksler: When patients come into the multidisciplinary clinic, patients / families with esophageal cancer will leave the office with a pretty good idea of what is going to happen. Depending on the work up done before they see me [which includes identification of tumor/ cancer staging], we will do the radiation therapy simulation the following
week, and start chemotherapy and/or radiation therapy the next week.
Question: What diagnostics/ medical records should they bring with them?
Dr. Weksler: We would like to see all available records, including previous surgeries, all scans, PET/ CT scans, barium esophagram, endoscopy report and all biopsy reports.
Question: What should patients anticipate? (will they get feeding tubes prior to surgery, etc)?
Dr Weksler: Most patients will get a port for chemotherapy*. We place feeding tubes in patients that loss more than 10% of their weight, or if they suffer from severe dysphagia. Patients can expect a 5 week course of chemotherapy and/or radiation therapy, followed by an interval of 6 to 8 weeks, followed by surgery.
*Editor’s note: A port is a long-term but temporary and completely removable central intravenous access for chemotherapy administration. It is placed underneath the skin with no cords, or lines visible externally. Feeding tubes are also temporary tubes that are easily removed/ reversible but help the patient to maintain adequate nutrition necessary for healing.
He has multiple offices including the West Cancer Center. For an appointment, please contact 901-448-2918.
Unfortunately, while Dr. Weksler and his thoracic surgery program are state-of-the-art, the Methodist website is not.
Additional references and resources (this is a selective list)
1. Oncologic efficacy is not compromised, and may be improved with minimally invasive esophagectomy.
Berger AC, Bloomenthal A, Weksler B, Evans N, Chojnacki KA, Yeo CJ, Rosato EL. J Am Coll Surg. 2011 Apr;212(4):5606; discussion 5668. doi: 10.1016/j.jamcollsurg.2010.12.042. PMID: 21463789
2. Outcomes after minimally invasive esophagectomy: review of over 1000 patients.
Luketich JD, Pennathur A, Awais O, Levy RM, Keeley S, Shende M, Christie NA, Weksler B, Landreneau RJ, Abbas G, Schuchert MJ, Nason KS. Ann Surg. 2012 Jul;256(1):95103.
doi: 10.1097/SLA.0b013e3182590603. PMID: 22668811 Free PMC Article – attached. Recommended reading. If you are only going to read one article on MIE, this is a nice project looking at a large number of patients.
3. Major perioperative morbidity does not affect long-term survival in patients undergoing esophagectomy for cancer of the esophagus or gastroesophageal junction.
Xia BT, Rosato EL, Chojnacki KA, Crawford AG, Weksler B, Berger AC. World J Surg. 2013 Feb;37(2):40815. doi: 10.1007/s0026801218236.
PMID: 23052816
4. The revised American Joint Committee on Cancer staging system (7th edition) improves prognostic stratification after minimally invasive esophagectomy for esophagogastric adenocarcinoma.
Zahoor H, Luketich JD, Weksler B, Winger DG, Christie NA, Levy RM, Gibson MK, Davison JM, Nason KS. Am J Surg. 2015 Oct;210(4):6107.
doi: 10.1016/j.amjsurg.2015.05.010. Epub 2015 Jun 26. PMID: 26188709
5. Minimally invasive esophagectomy in a 6 year-old girl for the sequelae of corrosive esophagitis.
Majors J, Zhuge Y, Eubanks JW 3rd, Weksler B. J Thorac Cardiovasc Surg. 2016 Jun 22. pii: S00225223(
16)305657. doi: 10.1016/j.jtcvs.2016.06.011. [Epub ahead of print] No abstract available.
PMID: 27406439
Cirugia de torax invites readers for an open discussion on the latest STS guidelines on multimodality treatment of esophageal cancer.
Guidelines for esophageal cancer?
Guidelines, guidelines, guidelines.. It seems like much of American medicine is now directed by guidelines, committees and government agencies. We have pay-for-performance, “Core Measures” and even more guidelines, recommendations and requirements that attempt to pre-script the care that we provide. This often leaves clinicians and surgeons feeling more like technicians following recipes for “cookbook medicine” to treat anonymous, “standardized” patients rather than highly skilled, extensively trained and experienced medical providers using clinical judgment, intellect and training to treat unique individuals.
Guideline fatigue, questionable “evidence” and mandated medicine
With that in mind, many healthcare providers are sick of reading and writing about “evidence-based practice recommendations and clinical guidelines”. Some of this frustration comes from the sometimes contradictory clinical evidence regarding these mandates, such as pre-operative beta blockade. While this medication is now mandated by the federal government, multiple studies* question the benefit of this treatment in patients undergoing noncardiac surgery.
As the debate continues to rage over this therapy, is it fair that surgeons must continue to risk their hospital’s performance scores, and surgical reimbursement for challenging the blanket administration of this medication to their patients?**
Not all guidelines created equally
The concept of clinical guidelines have its origins in the 1960’s. While differing political camps explain the emergence of these guidelines according to their individual bias (insurance cost-cutting versus autonomy etc.), it seems obvious that these guidelines were at least, initially, designed to improve the overall care of patients with similar diagnoses, symptoms or clinical scenarios.
But when it comes to these clinical guidelines – not all guidelines are created equally. In addition to criticism that many clinical guidelines are poorly supported by the existing literature, or based on poor quality studies, allegations of cronyism, obvious bias/ self-serving have plagued guideline committees particularly in the field of cardiology.
But what does this mean for thoracic surgery? We have our own organizational committees such as the Society for Thoracic Surgeons, (aka STS), our own recommendations, guidelines and ratings systems (national and international database). STS and thoracic surgery based clinical guidelines address the very lifeblood of our specialty and our clinical practice.
It behooves us as a professional specialty to read, review and know these guidelines so that we can determine when and if these guidelines serve our practices and our patients. If not, as representatives of thoracic surgery; it is our responsibility to participate and to voice our concerns and criticisms of these guidelines. We are the watchdogs, to prevent the over-representation of commercial interests or bias into our arena of patient care.
It is also crucial that we attempt to support the crafting of recommendations to support and adopt the best practices in thoracic surgery; after all, as practicing clinicians, we know thoracics better than any outside agencies, organizations or other specialties. With this philosophy in mind, Cirugia de Torax invites readers to become more familiar with the latest STS guidelines.
Society of Thoracic Surgeons guidelines
Thus far, the Society of Thoracic Surgeons has published eighteen guidelines on a wide variety of topics’ from antibiotic use, to cerebral protection of infants undergoing cardiac surgery, the use of TMR, to the newest guidelines on the treatment of esophageal cancer.
Cirugia de Torax would like to invite our American and International readers to participate in a review of the most recent guidelines in our next post. What do you think of trend towards guidelines in general? What about the guidelines for multi-modality treatment in esophageal cancer? Love them? Hate them? Any omissions or errors? Any changes or suggestions for future versions?
Deadline for submission of commentary, criticism or other remarks is January 15, 2015.
Notes:
* Link requires (free) subscription
** Surgeons can document a ‘variance’ on a case-by- case basis when omitting this and other prescribed core measures under a limited set of circumstances.
Article for Review
The Society of Thoracic Surgeons Practice Guidelines on the Role of Multimodality Treatment for Cancer of the Esophagus and Gastroesophageal Junction.
Little, Alex G. et al. (2014). The Annals of Thoracic Surgery , Volume 98 , Issue 5 , 1880 – 1885. pdf version.
Additional reference articles
1. Weisz G1, Cambrosio A, Keating P, Knaapen L, Schlich T, Tournay VJ. (2007). The emergence of clinical practice guidelines. Milbank Q. Dec;85(4):691-727.
2. The Society of Thoracic Surgeons Esophageal Cancer Guideline Series. Mitchell, John D. et al. The Annals of Thoracic Surgery , Volume 96 , Issue 1 , 7
3. The Society of Thoracic Surgeons Guidelines on the Diagnosis and Staging of Patients With Esophageal Cancer. Varghese, Thomas K. et al. The Annals of Thoracic Surgery , Volume 96 , Issue 1 , 346 – 356
Copies of all STS guidelines are available on-line here.
Is the Sweet esophagectomy still relevant in this era?
The Sweet esophagectomy, which was first described in 1942 by surgeon Richard H. Sweet has fallen out of popular practice in many locations in the world. It has been replaced by the more extensive Ivor- Lewis approach, as well as more recent developments including minimally invasive techniques.
Now, Jua Ma et al. (2014) argue that the Sweet esophagectomy remains relevant in the minimally invasive surgery era.
The Sweet Technique
Dr. Richard Sweet was not the first surgeon to perform a successful esophagectomy for cancer. As discussed in A. P. Naef’s series on the history of thoracic surgery, that distinction belongs to Dr. Franz Torek who performed what would become the “Torek” technique back in 1913.
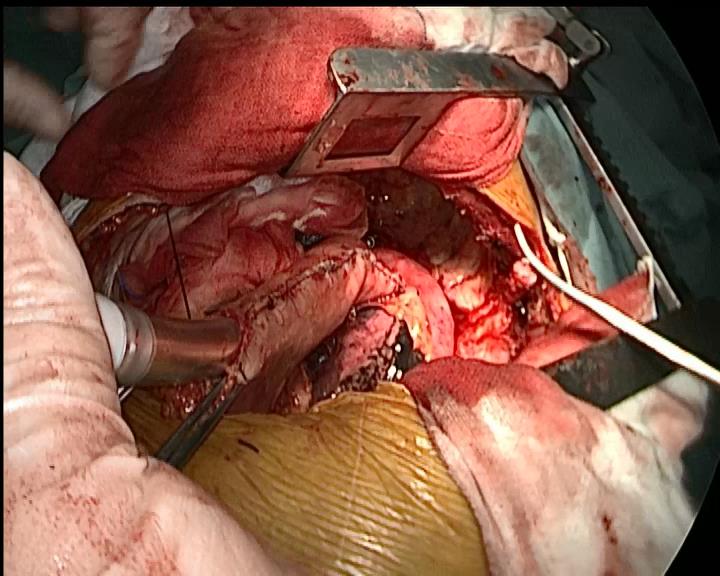
all intra-operative photos courtesy of Dr. Qun Wang, Fudan Univeristy, Zhongshan Hospital
However, it was Dr. Sweet’s modifications to this technique as well as numerous successes with this procedure that ushered in a new era of esophagectomies and successful esophageal surgery. In his hey-day, Dr. Sweet was also heralded for the speed of his procedure, which at under two hours was just half the time of many of his contemporaries.
What makes the Sweet esophagectomy different from the ‘modern’ techniques practiced today is the use of a sole left thoracotomy incision. (Versus the Ivor-Lewis with a right thoracotomy and midline laparotomy as well as the multiple port approaches, the Chen esophagectomy, not withstanding**).
(**In esophageal cancer, the need for extensive lymph node dissection for intra-operative staging often precludes the use of minimally invasive procedures). At present, the Ivor – Lewis approach remains the primary operation for esophageal cancer.
left posterolateral thoracotomy (illustration courtesy of Office of Military History)
As described by Jua Ma et. al, the standard incision is a posterolateral thoracotomy incision at the 5th or 6th intercostal space. After entering the chest cavity, the esophagus is dissected at least 5 cm above the lesion to allow for adequate surgical margins post-resection.
Care is taken to avoid trauma or damage to surrounding structures such as the thoracic duct, recurrent laryngeal and vagus nerves.
Once the esophagus was dissected completely from surrounding tissue, a 5 to 6cm incision was made into the diaphragm (which separates the thoracic and abdominal cavities). From here, surgeons can readily and easily enter the abdominal compartment to free the stomach for eventual anastomosis to the remaining portion of the esophagus.
Blood flow to the stomach is maintained by preserving the right gastro-epilotic arteries while the left gastric artery and vein are ligated for mobilization.
Complete abdominal lymph node dissection is completed with en-bloc dissection of distal esophagus and proximal stomach. The anastomosis itself is performed either above or below the aortic arch.
Good visualization while mobilizing the stomach during Sweet esophagectomy
As you can see from the photos included, this incision allows easy access to both the thoracic and abdominal cavities.
The Zhongshan experience
In this retrospective study involving patients undergoing esophagectomies for middle or lower esophageal carcinomas from January 2007 to December 2010, the authors were able to include 784 patients who had surgery via the Sweet approach versus 167 patients who underwent the Ivor – Lewis esophagectomy.
Exclusions
Patients who were inoperable due to the presence of mediastinal disease at the time of diagnosis and well as patients with high level lesions (located above the carina*) were excluded from the study.
*One of the drawbacks of the Torek – Sweet type procedures is the risk of phrenic nerve injury with high level lesions.
Patients undergoing other types of esophageal surgery such as cervical approaches or minimally invasive procedures were also excluded from this study. (Table 1 of the original article gives full details regarding surgical approaches for 1,138 patients having esophageal surgery at Zhongshan Hospital during this time period.)
Extensive experience
Most notable from a technical aspect of this study is the surgical experience of the surgeons involved. Each of the surgeons in this study had performed over 100 esophagectomies before initiating this investigation. As demonstrated numerous times in the scientific literature, the surgical experience of the surgeon as well as the oncological surgical volume of individual facilities play a significant role in patient outcomes.
Results
Overall:
Patients followed for 24 to 72 months. Out of 915, complete follow-up data was collected from 618 patients. (Patient attrition due to loss of follow-up, death etc. was accounted for in this study).
21 patients found to have metastasis (celiac lymph nodes) during lymph node dissection.
There was no different in the number of nodes dissected with either approach, however, there was a higher number of positive nodes in patients undergoing Ivor-Lewis with an open laparotomy. (28.7 % versus 38.7% with Ivor Lewis). Despite this finding – there was no significant different in the total number of metastasis in either approach – Sweet 42.5% and Ivor Lewis 45.2%
No difference in overall 5 year survival rate for either procedure.
Operative mortality was similar in both groups (2.3% for Sweet, Ivor Lewis 1.8%)
Sweet versus Ivor Lewis
– Shorter surgical time with Sweet approach (181 min +/-71 minutes) versus 208 minutes for Ivor Lewis (+/- 63 minutes).
– Less blood loss (and less transfusions) with Sweet approach
– Fewer complications
Overall rate of complications: Sweet 12.3%. One fifth of all Ivor Lewis (IL) patients experienced post-operative complications (20.4%)
wound infection: Sweet 3.2% IL 7.8%
delayed gastric emptying: Sweet 1.7% IL 4.7%
Anastomotic leak: Sweet 2.1% IL 4.2%
– Shorter length of stay
Average length of stay was 13.2 days for patients undergoing the Sweet procedure compared to 17.3 days for the Ivor Lewis group.
In addition, while only 4.4% of the Sweet group remained hospitalized for more than 30 days after surgery, 12.6% of the Ivor Lewis patients had a length of stay greater than 1 month.
Discussion
More positive nodes, but Why?
The increased finding of positive lymph nodes in patients undergoing the Ivor Lewis merits further discussion and investigation as to whether this is related to the areas of lymph node dissection since the authors discuss the difficulty of assessing areas of the anterior mediastinum. There is no mention of how using a single incision technique and accessing the stomach via the diaphragm affected abdominal lymph node dissection.
While the actual numbers harvested using either technique were comparable, were the surgeons able to harvest more lymph nodes from specific sites in the patients with an open laparotomy?
If so, this supports the notion that for some cancer operations, like this one, where accurate staging is absolutely essential for determining prognosis – open surgery may remain superior to “lesser” procedures such as the Sweet or minimally invasive approaches.
More importantly, the surgeons at Zhongshan illustrate both the magnitude of a surgical procedure like the Ivor Lewis and the potential benefits of alternative approaches performed by experienced surgeons.
Fewer anastomosis leaks
In their facility, patients experienced demonstrated only half the rate of wound infection with only one primary incision versus the two incision Ivor Lewis. More importantly, the incidence of a potentially lethal complication like anastomotic leak was also half (2.1%) of that for Ivor Lewis (4.2%**). While some of the literature has cited a mortality rate as low as 3.3% due to advances in the treatment of the associated sepsis, anastomotic leak remains a devastating complication.
**This rate mirrors what is seen in the literature for Ivor Lewis esophagectomies. The cited mortality for anastomotic leaks varies widely.
Limitations
The biggest limitation of this study is the retrospective design. However, at present, researchers (Dr.Haiquan Chen) at Fudan University are conducting another ongoing clinical trial to compare these procedures. This study is a prospective, randomized design.
Implications / considerations
The work done by Jua Ma et al. warrents careful reading and consideration; Zhongshan Hospital in Shanghai, China has over 1700 beds, and serves a large patient population, in which esophageal cancer is relatively common. The elevated incidence of esophageal cancer in China has been noted as far back as 2,000 years ago by Chinese scholars and physicians.
photo courtesy of echinacities.com
The increased incidence and presentation of patients with surgically resectable esophageal cancers combined with a robust thoracic surgery division (with over 29 thoracic surgeons on staff) provides the authors with an opportunity to collect, analyze and present data on a scale unheard of in the majority of institutions performing single-site investigation. In 2013, for example, the thoracic surgery department performed over 1152 Lung procedures and 683 esophageal procedures.
Sweet R. H. (1946). Subtotal esophagectomy with high intrathoracic esophagogastric anastomosis in the treatment of extensive cicatricial obliteration of the esophagus. Surg Gynecol Obstet. 1946 Oct;83:417-27.
Talking with Sandra Ogawa, ACNP about ‘What to do when the purple pill fails?”
Phoenix, Arizona
During my visit with Dr. Bremner at St. Joseph’s Hospital, I had the pleasure of meeting several members of the thoracic surgery team, including Sandy Ogawa.
Ms. Ogawa is an acute care nurse practitioner specializing in Thoracic Surgery. She initially began working with Dr. Bremner at USC as a nurse coordinator, and has been working with Dr. Bremner since he was a thoracic surgery fellow. After returning to school for her master’s degree – Ms. Ogawa became a nurse practitioner in thoracic surgery.
Since then she has taken on a wide range of duties and responsibilities caring for thoracic surgery patients, with a keen interest in anti-reflux procedures such as the Nissen fundaplication and the Toupet procedure.
One of the things we talked about was her upcoming presentation on proper patient selection and patient referral, or as Ms. Ogawa states, “What to do when the purple pill fails?”
Who should consider surgery for reflux?
The best patients for surgical treatment of reflux are patients who have failed first-line medical treatments such as Nexium (or other proton pump inhibitors.) Patients should explore these options as well as standard medical recommendations such as weight loss, and dietary modification prior to seeking the advice of a surgeon.
Symptoms & Complications of Reflux
Symptoms of GERD are varied and can range from simple heartburn to dysphagia (difficulty swallowing), chest pain, respiratory infections and dental erosion. Uncontrolled gastric reflux has been shown to negatively impact the patient’s quality of life; through interrupted sleep, impaired eating and other activities of daily living.
At St. Joseph’s, Dr Bremner and his colleagues specialize in both of these procedures (Nissen fundaplication and Toupet procedure) as well as re-do procedures for patients with re-current symptoms or re-current hernias after surgery.
Pre-surgical Evaluation: Diagnosis & Testing
Having ‘heartburn’ alone isn’t the only factor to consider prior to undergoing an anti-reflux procedure. The are multiple physiological factors that also help surgeons determine whether surgery is an appropriate treatment, and which surgical procedure is the best surgical option.
As part of their anti-reflux program, all pre-operative evaluation procedures (endoscopy with four quadrant biopsies, barium esophagrams, and manometry are performed in-house. In fact, the department has their own manometry lab, where they read all of their studies (versus sending patients to multiple departments). These tests help determine whether reflux is related to different conditions such as the presence of a hiatal hernia, or a malfunctioning esophageal sphincter. It is also important to rule out other causes of symptoms such as dysphagia such as an esophageal stricture since this condition is treated differently. If there is acid damaged tissue (tissue changes in the esophagus and stomach due to acid erosion), biopsies of the tissue will be taken to rule out Barrett’s esophagus or esophageal cancer.
Guess we’ll have to wait for the rest of Ms. Ogawa’s presentation to hear more.
Additional Resources: Anti-reflux procedures, GERD and treatment strategies
Talking with Dr. Ross Bremner, Chief of Thoracic Surgery and Chair of Thoracic Disease & Transplant at St. Joseph’s Hospital in Phoenix, Arizona.
Dr. Ross Bremner
St. Joseph’s Hospital
After talking to Dr. Bremner of the phone, I felt compelled to come down to Phoenix and meet him in person. I am glad I did. While St. Joseph’s is a large 607 bed hospital – it’s just one of many large healthcare facilities in the Phoenix area. The same can not be said of their robust thoracic surgery program. They have a surprising range of thoracic surgery subspecialties, and sub-specialty programs including transplant, anti-reflux surgery, minimally invasive surgery, esophageal surgery program and robotic surgery. As you can imagine, I felt a bit like a kid in a candy store – so overwhelmed by the array of services, that my mind was just bursting with questions. (I rounded with the group and got to see the full spectrum of patients – including four recent post-transplant patients.) They also have a pediatric thoracic surgery program and plan to start a pediatric transplant program soon.
Dr. Ross Bremner & Dr. Mike Smith, Heart & Lung Institute
The head of the program, Dr. Ross Bremner is one of five thoracic surgeons at the Heart & Lung Institute of St. Joseph’s Hospital in Phoenix, Arizona which is currently the state’s largest thoracic surgery program. A native of Johannesburg, Dr. Bremner maintains international ties to his home country by staying active in the South African Cardiothoracic Surgery Society. He began his thoracic surgery career at University of Southern California (USC) where he met and recruited both Dr. Michael Smith, MD and Sandra Ogawa, ACNP.
As Arizona has grown, so has thoracic surgery. Despite the relatively small population of Arizona overall, both the esophageal surgery program and the lung transplant program maintain volumes that are competitive with the big-name east coast institutions.
With over 45 lung transplants last year – and the University of Arizona currently out of the running, Dr. Bremner* and his team are set to boost those numbers this year. They have already done ten transplants here in the first quarter of 2012, and anticipate doing fifty to sixty this year. (If you remember from our previous posts about lung transplantation – even very large institutions are not doing huge numbers of transplants. In fact, you can check the numbers at the Organ Procurement and Transplant Network if you’re interested*.)
St. Joseph’s also has an esophageal surgery program which maintains the high volumes of esophagectomies needed for optimal outcomes. Dr. Bremner reports that they perform on average 50 – 60 esophagectomies for esophageal cancer ever year in addition to their benign esophageal surgery program. (As we discussed with Dr. Molena, ‘benign’ is a bit of a misnomer for esophageal conditions since achalasia, esophageal strictures and other non-cancerous conditions of the esophagus may have a huge negative impact on the individual’s quality of life.)
The Heart & Lung Institute also offers training courses for surgeons and residents in minimally invasive surgery – in fact, they are teaching a course the weekend of my visit.
As a practicing surgeon in Phoenix, Arizona, Dr. Bremner also sees numerous cases of Coccidoidomycosis** (or Valley Fever) which is endemic to this area of the country. In fact, Maricopa county, which encompasses the city of Phoenix sees more cases annually than the California valley the disease was originally named for.
* At the site, you can create data reports by organ, region, outcome, waiting period, etc.. For example – using this data table – we can see that there were a total 1,516 isolated lung transplants in the United States in 2011 which is actually a decrease from 2010 and 2009.
** Readers can anticipate a future article on this topic
Dr. Bremner is a genial gentleman and a ready conversationalist. Our interview was relaxed, but informative. He welcomed my questions on a variety of topics and was generous with his time. In fact, I had ready access to multiple members of his team, and spent the entire afternoon with the department of thoracic surgery. It was an engaging afternoon, and highlighted one of the reasons I pursue interviews and opportunities to speak to my colleagues within thoracics; it was an opportunity to learn more about the specialty, and the care of thoracic surgery patients.
Dr. Bremner is a board-certified thoracic surgeon. After obtaining his baccalaureate degree and medical school training at Witwatersrand University in South Africa, he continued his education in the United States.
He completed his general surgery residency, PhD research and thoracic surgery residency at the University of Southern California. He was the Director of the Hastings Thoracic Oncology Research Laboratory on the USC campus. At this lab, surgeons along with researchers from multiple disciplines conduct research on the diagnosis and treatment of lung cancer including research in gene therapies prior to coming to Arizona.
He has several YouTube videos talking about his current research projects at St. Joseph’s.
He also has an informational series for patients about Lung Transplant over at EmpowHer.com
Dr. Ross M. Bremner, MD, PhD
Chief of Thoracic Surgery
Chair of the Center for Thoracic Disease & Transplantation
Heart & Lung Institute – St. Joseph’s Hospital and Medical Center
500 W. Thomas Road, Suite 500
Phoenix, Arizona 85013
Tele: (602) 406 4000
Fax: (602) 406 3090
Selected publications (not a full listing)
Jacobs JV, Hodges TN, Bremner RM, Walia R, Huang J, Smith MA. (2011). Hardware preservation after sternal wound infection in a lung transplant recipient. Ann Thorac Surg. 2011 Aug;92(2):718-20. [no free text available].
Felton VM, Inge LJ, Willis BC, Bremner RM, Smith MA. (2011). Immunosuppression-induced bronchial epithelial-mesenchymal transition: a potential contributor to obliterative bronchiolitis. J Thorac Cardiovasc Surg. 2011 Feb;141(2):523-30. [no free text available].
Backhus LM, Sievers E, Lin GY, Castanos R, Bart RD, Starnes VA, Bremner RM. (2006). Perioperative cyclooxygenase 2 inhibition to reduce tumor cell adhesion and metastatic potential of circulating tumor cells in non-small cell lung cancer. J Thorac Cardiovasc Surg. 2006 Aug;132(2):297-303. [no free full-text available].
Backhus LM, Sievers EM, Schenkel FA, Barr ML, Cohen RG, Smith MA, Starnes VA, Bremner RM. (2005). Pleural space problems after living lobar transplantation. J Heart Lung Transplant. 2005 Dec;24(12):2086-90. [no free text available].
Backhus LM, Petasis NA, Uddin J, Schönthal AH, Bart RD, Lin Y, Starnes VA, Bremner RM. (2005). Dimethyl celecoxib as a novel non-cyclooxygenase 2 therapy in the treatment of non-small cell lung cancer. J Thorac Cardiovasc Surg. 2005 Nov;130(5):1406-12. [no free full-text available].
Sievers EM, Bart RD, Backhus LM, Lin Y, Starnes M, Castanos R, Starnes VA, Bremner RM. (2005). Evaluation of cyclooxygenase-2 inhibition in an orthotopic murine model of lung cancer for dose-dependent effect. J Thorac Cardiovasc Surg. 2005 Jun;129(6):1242-9. [no free full-text available].
Bowdish ME, Barr ML, Schenkel FA, Woo MS, Bremner RM, Horn MV, Baker CJ, Barbers RG, Wells WJ, Starnes VA. (2004). A decade of living lobar lung transplantation: perioperative complications after 253 donor lobectomies. Am J Transplant. 2004 Aug;4(8):1283-8. [no free full-text available].
A review of recently published articles on the risk factors and early detection of esophageal cancer.
Last year, while researching a book in Latin America, I had the good fortune to meet Dr. Fabian Emura. Unlike most physicians profiled here at Cirugia de Torax.org, Dr. Emura is not a thoracic surgeon. Dr. Emura is a gastroenterologist specializing in the early detection of digestive cancers, including esophageal cancer. Dr. Emura, and other doctors like him, use a diagnostic technique called chromoendoscopy to identify early gastric, esophageal and colonic lesions in high risk patients. This is particularly important in gastric cancers such as esophageal and stomach cancers. These cancers are usually not detected until late stage disease when the patients develop symptoms such as dysphagia (inability to eat), anorexia, weight loss, nausea, early satiety or a feeling of abdominal fullness.
However, the development of chromoendoscopy, which is a fairly inexpensive technique that involves using a dye (Lugol’s) to detect abnormal cells in esophageal (and gastric mucosa.) The areas of abnormality will fail to change color when dye is applied. This technique, combined with narrow band imaging and other diagnostic modalities can aid in the early diagnosis of esophageal cancers.
Who should get tested?
As we discussed in a previous post, the incidence of adenocarcinoma based esophageal cancers is rising dramatically. Unlike esophageal cancer from squamous cell carcinoma, the risk factors for squamous cell type vary from the traditional risk factors of smoking, alcohol ingestion, history of Barrett’s esophagus and geographic factors.
In comparison, a study by Yu et. al. found that contrary to common belief, coffee did not contribute to the development of esophageal (and other cancers) and this meta-analysis of over 500 published studies showed that coffee may actually be beneficial.
Anyone with the above mentioned risk factors of smoking, heavy alcohol ingestion, frequent or uncontrolled gerd (acid reflux), or a family history of esophageal cancer should consider additional testing. Anyone with unexplained weight loss, loss of appetite, dysphagia (difficulty eating or swallowing), or abdominal pain should seek prompt medical attention.
Neither this article or any information of this site should be used in lieu of medical attention/ evaluation or advice from a licensed medical provider.
at John Hopkins, talking with Dr. Daniela Molena about minimally invasive thoracic surgery.
Baltimore, Maryland
John Hopkin’s newest recruit to the Department of Thoracic Surgery, Dr. Daniela Molena is a bright point in the future of thoracic surgery. While she has only been at Hopkins for a few short months (since September) she is already innovating and bringing positive changes to the institution. In fact, there is too much to say about this fascinating and charming surgeon in just one article.
A practicing general surgeon in her native Italy, Dr. Molena rapidly became interested and proficient in the surgical treatment of benign esophageal diseases. As a specialist in diseases of the esophagus, she has extensive training in both gastrointestinal and thoracic surgery. Pursuit of this education brought her to the United States.
Once here, Dr. Molena took advantage of the opportunities to train with some of the most renown surgeons in the country; with Dr Marco Patti in San Francisco, with Dr Peters Jeffrey in Rochester, Memorial Sloan Kettering Cancer Center in NY with Dr Rusch Valerie and Dr. James Luketich at the University of Pittsburgh Medical Center, and now here at John Hopkins with Dr. Stephen Yang. She believes this gave her a better appreciation for all the different techniques and schools of though in thoracic surgery. “I don’t just use a specific surgeon’s approach, I can use the best I have learnt from each mentor and apply it to best fit the individual patient and their needs.”
Once she arrived here, she hit the ground running; gathering research on esophageal surgery; starting a lung cancer screening program for some of Baltimore’s more poverty-stricken communities, arranging for patient outreach sessions for cancer patients, working with Dr. Avo Meneshian’s robot-assisted thoracic surgery (RATS) program at the John Hopkins Bayview facility, and quickly advancing, promoting and heading a new program for minimally invasive esophageal surgery (including minimally invasive esophagectomy (MIE) for esophageal cancer). She favors the Ivor-Lewis style procedure but performs it via thoracoscopy and laparoscopic approaches. She thinks it is important to stress that minimally invasive surgery is just the approach or the tool to gain access to the chest to complete a surgical procedure. Thus, a minimally invasive procedure does not mean a lesser or inferior resection. “It’s how we get in – once we get in [to the chest], we can do whatever surgery is needed, respecting oncologic principles.”
While the MIE program is young, Dr. Daniela Molena hopes to grow this program with time, as part of a multi-disciplinary program for esophageal cancer patients. This holistic approach which combines diagnosticians, oncologists, dietitians, nutritionists, nurses, and surgeons is also an immensely practical one. This multi-specialty clinic ensures that the patient/ and their family is able to meet with, consult with and work collaboratively with all of these specialties to determine their course of treatment on the same day during a single trip. This alleviates much of the financial and transportation hardships experienced by many of the families travelling from around the country (and around the world[1]) for treatment at John Hopkins.
Dr. Molena takes this holistic approach to thoracic disease very seriously. As she explains, “Even benign (non-cancerous) esophageal diseases are terrible for patients and their families. They have to learn to adapt and accept that even with treatment, life may never be the same”. She feels that it is essential that we speak to patients openly, and honestly and set realistic expectations, stating “People, especially our patients, are remarkably resilient if we communicate clearly with them during this process.” She also feels that as a surgeon she is here to do more for her patients that operate, that it’s not just about cutting. She is here to help patients (and their loved ones) find all the resources they need to regain optimal health and promote wellness. “It is more than just surviving the surgery. It’s about health & wellness,” she finishes.
It’s a strong, profound statement and a reminder for surgery but one that reflects the thoughts and feelings of many of the wonderful thoracic surgeons I have met, interviewed or worked with. But in Medicine, with many of it’s rigid definitions and delineations; too often the surgeons themselves, their motivations, and their desire to heal gets lost among the surgeries, and the procedures.
Medical School: Faculty of Medicine University of Padova (Padova Italy)
(1996)
General Surgery residencies:
University of Rochester Medical Center (Rochester NY) – General Surgery (2009)
Faculty of Medicine University of Padova (Padova Italy) – General Surgery (2001)
Faculty of Medicine University of Padova (Padova Italy) – General Surgery (1999)
Fellowships:
Memorial Sloan-Kettering Cancer Center (New York NY) – Cardiothoracic Surgery (2011)
University of Pittsburgh Medical Center (Pittsburgh PA) – Cardiothoracic Surgery (2010)
New York Presybterian Hospital (New York NY) – Cardiothoracic Surgery (2011)
Memorial Sloan-Kettering Cancer (New York NY) – Cardiothoracic Surgery (2009)
Universita Degli Studi di Padova (Padova Italy) – Minimally Invasive Surgery (2002)
[1] John Hopkins has a separate department called the International Patient Center which is devoted to detangling and simplifying the health care process for overseas patients.
Williams VA, Watson TJ, Gellersen O, Feuerlein S, Molena D, Sillin LF, Jones C, Peters JH. Gastrectomy as a remedial operation for failed fundoplication. J Gastrointest Surg. 2007 Jan;11(1):29-35. [no free full-text available].
A brief discussion of the variety of surgical approaches used for esophagectomy for esophageal cancer including Ivor Lewis, Transhiatal and minimally invasive techniques.
An esophagectomy is surgical resection of the esophagus. If this includes the upper portion of the stomach (for cancers in the distal third) it is sometimes called an esophagogastrectomy. This procedure is often performed as part of treatment for early stage esophageal cancers. This procedure is technically challenging and requires advanced surgical skill and training in esophageal surgery. The general consensus among surgeons and published literature is that a surgeon needs to perform a minimum of 12- 25 esophagectomies per year to maintain proficiency.
Who does the most esophageal surgeries in the USA? The University of Pittsburgh (UPMC) and Dr. Benny Weksler*.
There are several surgical approaches for this procedure, and the “best” approach is a topic that is widely debated among thoracic surgeons. As technology continues to advance, and newer techniques emerge, esophagectomy/ esophagogastrectomy continues to evolve.
Ivor Lewis Esophagectomy
The Ivor Lewis esophagectomy or the transthoracic approach is considered the ‘Gold standard’ among many thoracic surgeons. Named for the surgeon that popularized this approach in 1946, this surgical procedure is actually a combination of two separate surgical procedures – a laparotomy incision to allow for mobilization of the stomach, and a right-sided thoracotomy for excision and resection of the esophagus. In the modified approach discussed by David & Marshall (2010), the need for patient repositioning in eliminated, allowing for a faster, more efficient operation without sacrificing visibility or accessibility for lymph node dissection. (During the standard approach – the patient is re-positioned after the laparotomy portion of the operation is complete.)
* The presence of metastatic disease drastically changes longevity outcomes, and makes esophagectomy ineffective for cancer treatment.
The main disadvantage is that the Ivor Lewis approach is a big operation (actually two operations) and carries the complications of both a large abdominal operation and a large thoracic procedure (with a thoracotomy.) One of these complications is increased pain. In addition to being burdensome for the patient to endure, the increased pain leads to increased pneumonias, respiratory and other complications due to ineffective pulmonary toileting and limited mobility secondary to this discomfort.)
This procedure is contraindicated in patients who have undergone a previous thoracotomy (due to adhesions). As alluded to above, all surgical resections (Ivor Lewis, Transhiatal and other approaches) are contraindicated in patients with evidence of metastatic disease.
Cerfolio, R. J., Bryant, A. S., Bass, C. S., Alexander, J. R. & Bartolucci, A. A. (2004). Fast tracking after Ivor Lewis esophagogastrectomy.Chest 2004 Oct; 126 (4) 1187 – 94. As the article explains – another advantage of high volume centers is fast-tracking after surgery for a day seven (POD#7) discharge. This also promotes standardization of care which is essential in teaching facilities and other healthcare centers with residents/ students/ frequent staff turnover.
The transhiatal approach was first discussed in the literature in 1933, but fell out of favor for a number of years before making a resurgence in the 1970’s.
In the transhiatal approach, the surgeon still makes two separate incisions – one in the anterior cervical area (neck) and a laparotomy for mobilization of the stomach. The main advantage to this approach is the avoidance of a thoracostomy incision, and a shorter duration of the operation. (The use of a thoracotomy incision is believed to increase the risk of post-operative pulmonary complications). The other advantages of the transhiatal approach are less pain (thoracotomy incision is more painful than cervical approach). This approach also eliminates the possibility of mediastinitis from an anastamotic leak since the anastamosis is not in the thoracic cavity.
However, detractors of this procedure cite the difficulties due to poor visualization of the esophageal tumors during the operation, the increased rate of anastamosis leak and development of post-operative strictures (Barreto & Posner, 2010).
Currently, there are several large randomized studies comparing newer surgical techniques with the Ivor Lewis esophagectomy. The MIRO trial and the TIME trials are on-going. (Enrollment in both of these trials are on-going with more information for interested patients available at clinicaltrials.gov).
There are multiple varieties of approaches for ‘minimally invasive’ esophageal surgery. These procedures are Ivor Lewis or Transhiatal approaches that have been modified by the use of laparoscopic equipment (for the abdominal portion) or thoracoscopic equipment for the transthoracic or transhiatal portion, or a combination of the above. Robot-assisted technologies have also been used in modified approaches to reduce incision size, (thus post-operative pain/ pulmonary complications.) A recent study by Dr. Luketich showed favorable outcomes in a large series of patients undergoing minimally-invasive procedures (link to article abstract below.)
Akiyama, S., Kodera, Y., Koike, M., Kasai, Y., et al. (2001). Small incisional esophagectomy with endoscopic assistance: evaluation of a new technique. Surgery Today, 31 (4) 378 – 382. [no free full text available.] Description of the ‘Akiyama’ approach.
Gao, Y., Wang, Y., Chen, L. & Zhao, Y. (2011). Comparison of open three-field and minimally invasive esophagectomy for esophageal cancer. Interact CardioVasc Thorac Surg 2011, 12: 366 – 369. I would have to argue against the authors contention that the McKeown approach is the preferred open surgical technique of most thoracic surgeons. (The McKeown is a modification of the Ivor Lewis). Surgeons: Care to comment?
Herbella, F. A., & Patti, M. G. (2010). Minimally invasive esophagectomy.World Journal of Gastroenterology,2010 Aug 14; 16 (30) 3811 – 3815.
James D Luketich, MD, Omar Awais, DO*, Manisha Shende, MD*, Neil A Christie, MD*, Benny Weksler, MD*, Rodney J Landreneau, MD, Blair A Jobe, MD*, Ghulam Abbas, MD*, Arjun Pennathur, MD*, Matthew J Schuchert, MD*, Katie S Nason, MD, MPH* University of Pittsburgh, Pittsburgh, PAOutcomes after minimally invasive esophagectomy. Presented at the 131 annual meeting of the American Surgical Association, April 14th – 16th, 2011 in Boca Raton, Fla.
a brief snapshot of a Dr. Benny Weksler, a thoracic surgeon using robotic technology at the University of Pittsburgh in Pittsburgh, Pennslyvania. Also, UPMC as a high volume esophagectomy center.
One of the prominent thoracic surgeons performing robotic procedures is Dr. Benny Weksler, a Brazilian native who is currently the Director of Robotic Thoracic Surgery at the University of Pittsburgh Medical Center in Pittsburgh, Pennslyvania*.
Dr. Weksler does a wide range of thoracic procedures using the daVinci robot including pulmonary lobectomies for cancer, esophagectomies for cancer, thymectomies for myasthenia gravis and thymoma, Heller myotomies for achalasia, Nissen fundoplications for GERD, repair of hiatal hernias, removal of mediastinal masses, correction of esophageal diverticula. He reports an overall annual surgical volume of approximately 450 cases, (with about 180 of these procedures using robotic technology.)
Dr. Benny Weksler, MD, FACS Associate Professor of Cardiothoracic Surgery Director, Robotic Thoracic Surgery University of Pittsburgh Medical Center Pittsburgh Pa.
Office Addresses:
Hillman Cancer Center
5115 Centre Avenue
Pittsburgh, PA 15232
Phone: (412) 648-6271
VA Medical Center
University Drive C
Pittsburgh, PA 15240
Phone: (412) 688-6000
Publications (an abbreviated selection of recently published works.)
Weksler B, Sharma P, Moudgill N, Chojnacki KA, Rosato EL. (2011). Robot-assisted minimally invasive esophagectomy is equivalent to thoracoscopic minimally invasive esophagectomy. Dis Esophagus. 2011 Sep 7. [no free full text available.]
Weksler B, Nason KS, Mackey D, Gallagher A, Pennathur A. (2011). Thymomas and Extrathymic Cancers. Ann Thorac Surg. 2011 Sep 30. [no free full text available].
Weksler B, Tavares J, Newhook TE, Greenleaf CE, Diehl JT (2011). Robot-assisted thymectomy is superior to transsternal thymectomy. Surg Endosc. 2011 Sep 5. [no free full text].
Berger AC, Bloomenthal A, Weksler B, Evans N, Chojnacki KA, Yeo CJ, Rosato EL. (2011). Oncologic efficacy is not compromised, and may be improved with minimally invasive esophagectomy. J Am Coll Surg. 2011 Apr;212(4):560-6; discussion 566-8. [no free full available]. Included since topic germaine to discussion.
Sivarajah M, Weksler B. (2010). Robotic-assisted resection of a thymoma after two previous sternotomies. Ann Thorac Surg. 2010 Aug;90(2):668-70. [no free full-text available].
* Dr. Weksler was kind enough to answer my questions in a series of emails. I did not have the opportunity to visit Dr. Weksler or his program on site.
the transoral esophagastric fundoplication procedure and Dr. Darren Rohan, a thoracic surgeon performing this minimally invasive technique.
A cardiothoracic surgeon in New York, Dr. Darren Rohan has started a new minimally invasive program for reflux surgery (called fundoplication.) With the transoral esophagogastric fundoplication procedure, he can tighten the sphincter (valve) between the stomach and the esophagus by endoscopy (instead of laparoscopic surgery) to prevent acid from refluxing into the esophagus. This is an important development in the treatment of gerd (gastroesophageal reflux disease) since the incidence of gerd is on the rise – due to obesity and this has led to an increase in esophageal cancer (as discussed in a previous post).
(Now, Dr. Rohan isn’t the first person to perform this procedure but I thought he’s be a great person to tell us more about it here at Cirugia de Torax, so I’ve written to him to request more information and to invite him to contribute a guest post.)
We also know that in addition to esophageal cancer (and Barrett’s esophagus) that reflux does more than destroy tooth enamel. Work by researchers at Duke has linked reflux with problems with lung transplant recipients, and then to reactive airway disease itself. While the degree of this relationship is not fully understood and is still debated – it is clear that there is a correlation to reflux disease and airway disease. It has also been associated with aspiration pneumonia, particularly in patients on reflux suppressing medications.
I’ll be updating this story soon with more information.
This 2009 review of the literature, by Kumar and Gupta out of India claims no association between reflux and asthma (but uses the effectiveness of acid suppressing medications in treating asthma as their proof of this theory – which is a faulty premise, in my opinion since these medications often don’t effectively treat reflux.)
More about the transoral esophagogastric fundaplication:
In an investigational study, Akutsu et. al. (2010) demonstrated a significant reduction in post-operative pneumonia through the implementation of a dental hygiene program.
A Japanese study suggests that one of the most important ways to reduce post-operative risk is also the easiest – by practicing good dental hygiene. While research has previously linked coronary artery disease (CAD) with dental plaque and chronic gum inflammation – two articles by Akutsu et. al (2010) in Japan have shown a reduction in post-operative pneumonia in esophageal cancer patients through the use of dental hygiene regimens.
The first of these articles in an overview of several factors to reduce post-operative risk, and was previously mentioned in another post:
Akutsu, Y. & Matsubara, H. (2009) Perioperative Management for the Prevention of Postoperative Pneumonia with Esophageal Surgery. Ann Thorac Cardiovasc Surg. 2009 Oct;15(5):280-5. (free full text). This is a well written report by Japanese surgeons on several techniques to reduce post-operative pneumonia. Several of these items can be directly implemented by patients – such as pre-operative smoking cessation, pulmonary rehabilitation and good dental hygiene.
The second article, “Pre-operative dental brushing can reduce the risk of post-operative pneumonia in esophageal cancer patients” was published in Surgery (2010, Apr; 147(4) 497-502.) The authors conducted an investigational study using 86 thoracic surgery patients scheduled to undergo esophagectomy. A control group of 41 patients and the dental hygiene (treatment) group consisting of 45 patients.
The dental hygiene group underwent no special dental procedures or cleanings but were instructed to brush their teeth five times a day.
The results showed a dramatic decrease in the incidence of post-operative pneumonia in the treatment group. 32% of the control group developed pneumonia post-operatively compared to only 9% of the toothbrushing group. 12% of the patients in the control group required tracheostomy due to the development of pneumonia (and prolonged respiratory support). No members of the treatment group required tracheostomy.
While the study size is relatively small – the results show an impressive reduction in post-operative pneumonia for a fairly small investment (increased tooth brushing/ dental hygiene.)
Discussion of article by Bilimoria and the importance of high volume esophageal surgery programs for successful post-operative outcomes.
Here’s another study highlighting the importance of having esophagectomies (esophageal surgery) at high volume centers. It’s a topic we’ve talked about before, and as it’s something I feel very strongly about – something readers will probably see mentioned again. It also helps answer the question – “Do I need to travel to X for surgery or can I have it at the local hospital?” This was the main questions the researchers were looking at for this study in terms of costs, logistics and burdens on patient and family.
This article by Bilimoria et. al (2010), published in the Annals of Surgery, was actually comparing outcomes for multiple surgery types at small community hospital versus large specialty center, not just thoracic surgeries but the research findings are similar to what we have reported previously. The irony of this study is that the researchers were expressly trying to prove the opposite, that small hospitals are safe for high complexity, high morbidity/ mortality operations – as a way to cut costs, and save money by preventing additional patient shifting to larger institutions that may be at a considerable distance for patients. They demonstrated limited success in their results for other surgeries – but the need for high volume esophagectomy programs for successful surgical outcomes remains unchanged. (Some of this may be due to the fact that many of these esophagectomies at smaller hospitals are performed by general, not thoracic surgeons.)
The answer for patients with esophageal cancer is: Yes – you do need to go to the esophageal cancer center (not your local community hospital). This is regardless of classification of low or high risk (which is based on age, and a Charlson score – which is a score used to add up other risk factors). This is something I have had to address with patients in my own personal practice as both a referring provider (at a smaller facility) and as a receiving provider (when I was at a larger esophageal surgery center.)
I’ve reposted the abstract below, so you can read for yourself. (The article itself is several pages long). [Italics are mine..]
Bilimoria, et. al. (2010). Risk-based Selective Referral for Cancer Surgery: A Potential Strategy to Improve Perioperative Outcomes Annals of Surgery. 2010;251(4):708-716.
Abstract
Background: Studies have demonstrated volume-outcome relationships for numerous operations, providing an impetus for regionalization; however, volume-based regionalization may not be feasible or necessary. Our objective was to determine if low-risk patients undergoing surgery at Community Hospitals have perioperative mortality rates comparable with Specialized Centers.
Methods: From the National Cancer Data Base, 940,718 patients from ~1430 hospitals were identified who underwent resection for 1 of 15 cancers (2003–2005). Patients were stratified by preoperative risk according to age and comorbidities. Separately for each cancer, regression modeling stratified by high- and low-risk groups was used to compare 60-day mortality at Specialized Centers (National Cancer Institute-designated and/or highest-volume quintile institutions), Other Academic Institutions (lower-volume, non-National Cancer Institute), and Community Hospitals.
Results: Low-risk patients had statistically similar perioperative mortality rates at Specialized Centers and Community Hospitals for 13 of 15 operations. High-risk patients had significantly lower perioperative mortality rates at Specialized Centers compared with Community Hospitals for 9 of 15 cancers. Regardless of risk group, perioperative mortality rates were significantly lower for pancreatectomy and esophagectomy at Specialized Centers. Risk-based referral compared with volume-based regionalization of most patients would require fewer patients to change to Specialized Centers.
Conclusions: Perioperative mortality for low-risk patients was comparable at Specialized Centers and Community Hospitals for all cancers except esophageal and pancreatic, thus questioning volume-based regionalization of all patients. Rather, only high-risk patients may need to change hospitals. Mortality rates could be reduced if factors at Specialized Centers resulting in better outcomes for high-risk patients can be identified and transferred to other hospitals.
There is a new trial on the horizon that sounds promising; the Traditional Invasive versus Minimally Invasive Esophagectomy (TIME). It’s a timely study indeed as the rates of esophageal cancer in western countries continues to increase, due to GERD and obesity.
I really don’t like the ‘cutesy’ way research trials have been named for the last ten years or so – but in this case – I will just have to look past it. There is a new trial on the horizon that sounds promising; the Traditional Invasive versus Minimally Invasive Esophagectomy (TIME) trial based in the Netherlands. It is a multi-center trial taking place at six hospitals in Europe. This trial will compare both morbidity and mortality in patients undergoing traditional esophagectomy (Ivor Lewis) and patients undergoing minimally – invasive (thoracoscopy combined with laparoscopy) after both sets of patients receive adjuvant chemotherapy. (This approach differs from the transhiatal esophagectomy developed at the University of Michigan in the 1970’s).
The researchers are planning for a five-year follow-up to compare both immediate post-operative complications / mortality with long-term effects (QoL) and cancer recurrence.
The full article is detailed on Medscape. (Also published in BMC Surgery. 2011;11 ). This couldn’t come at a more appropriate time, with recent data showing an abrupt rise in the incidence of esophageal cancer.
In an article (Chustecka) dated from September 2010, British researchers at Cancer Research UK reported a 50% increase in diagnoses of esophageal cancer in the last 25 years, particularly in men in their 50’s. (with an incidence of 14.4 men per 100,000, to put it into perspective, up from 9.9 in 1983.)
More concerning, is the fact that the prevalence of the types of cancer are changing. Previously, the majority of esophageal cancers were caused by squamous cell carcinoma which is linked to smoking and alcohol use. This study, along with an American study, shows an increasing incidence of adenocarcinoma, which is more commonly attributable to gastroesophageal reflux (Barrett’s esophagus). Researchers (Dr. Mark Orringer) estimate that the incidence of adenocarcinoma of the esophagus has increased by 350% in the last thirty years – and is directly related to huge increases in obesity. It now accounts for over 85% of esophageal cancers in the USA.
We’ll bring you more as the trial continues, and preliminary results are reported.
(Dr. Mark Orringer, who was quoted in the original medscape article from 2007 is one of several pioneering surgeons in thoracic surgery. He invented two of the surgical techniques in use today; the aforementioned transhiatal esophagectomy and the Collis -Nissen hiatal hernia repair.)