The Sweet esophagectomy, which was first described in 1942 by surgeon Richard H. Sweet has fallen out of popular practice in many locations in the world. It has been replaced by the more extensive Ivor- Lewis approach, as well as more recent developments including minimally invasive techniques.
Now, Jua Ma et al. (2014) argue that the Sweet esophagectomy remains relevant in the minimally invasive surgery era.
The Sweet Technique
Dr. Richard Sweet was not the first surgeon to perform a successful esophagectomy for cancer. As discussed in A. P. Naef’s series on the history of thoracic surgery, that distinction belongs to Dr. Franz Torek who performed what would become the “Torek” technique back in 1913.
However, it was Dr. Sweet’s modifications to this technique as well as numerous successes with this procedure that ushered in a new era of esophagectomies and successful esophageal surgery. In his hey-day, Dr. Sweet was also heralded for the speed of his procedure, which at under two hours was just half the time of many of his contemporaries.
What makes the Sweet esophagectomy different from the ‘modern’ techniques practiced today is the use of a sole left thoracotomy incision. (Versus the Ivor-Lewis with a right thoracotomy and midline laparotomy as well as the multiple port approaches, the Chen esophagectomy, not withstanding**).
(**In esophageal cancer, the need for extensive lymph node dissection for intra-operative staging often precludes the use of minimally invasive procedures). At present, the Ivor – Lewis approach remains the primary operation for esophageal cancer.

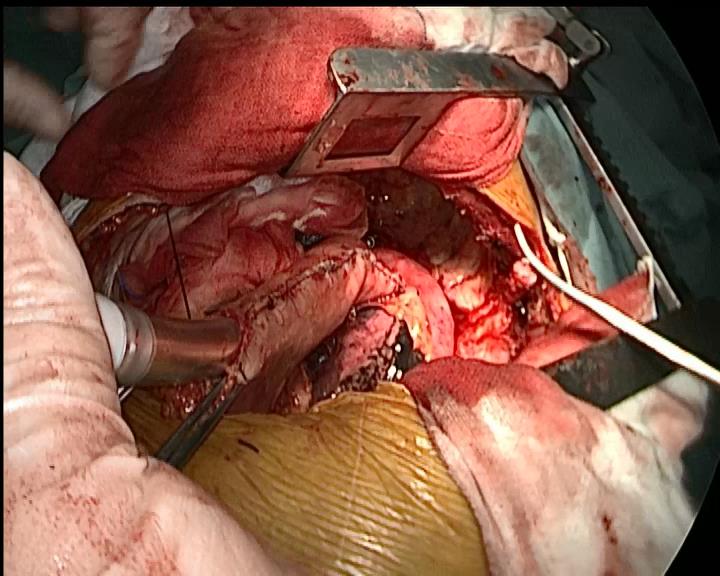
As described by Jua Ma et. al, the standard incision is a posterolateral thoracotomy incision at the 5th or 6th intercostal space. After entering the chest cavity, the esophagus is dissected at least 5 cm above the lesion to allow for adequate surgical margins post-resection.
Care is taken to avoid trauma or damage to surrounding structures such as the thoracic duct, recurrent laryngeal and vagus nerves.
Once the esophagus was dissected completely from surrounding tissue, a 5 to 6cm incision was made into the diaphragm (which separates the thoracic and abdominal cavities). From here, surgeons can readily and easily enter the abdominal compartment to free the stomach for eventual anastomosis to the remaining portion of the esophagus.
Blood flow to the stomach is maintained by preserving the right gastro-epilotic arteries while the left gastric artery and vein are ligated for mobilization.
Complete abdominal lymph node dissection is completed with en-bloc dissection of distal esophagus and proximal stomach. The anastomosis itself is performed either above or below the aortic arch.

As you can see from the photos included, this incision allows easy access to both the thoracic and abdominal cavities.
The Zhongshan experience
In this retrospective study involving patients undergoing esophagectomies for middle or lower esophageal carcinomas from January 2007 to December 2010, the authors were able to include 784 patients who had surgery via the Sweet approach versus 167 patients who underwent the Ivor – Lewis esophagectomy.
Exclusions
Patients who were inoperable due to the presence of mediastinal disease at the time of diagnosis and well as patients with high level lesions (located above the carina*) were excluded from the study.
*One of the drawbacks of the Torek – Sweet type procedures is the risk of phrenic nerve injury with high level lesions.
Patients undergoing other types of esophageal surgery such as cervical approaches or minimally invasive procedures were also excluded from this study. (Table 1 of the original article gives full details regarding surgical approaches for 1,138 patients having esophageal surgery at Zhongshan Hospital during this time period.)
Extensive experience
Most notable from a technical aspect of this study is the surgical experience of the surgeons involved. Each of the surgeons in this study had performed over 100 esophagectomies before initiating this investigation. As demonstrated numerous times in the scientific literature, the surgical experience of the surgeon as well as the oncological surgical volume of individual facilities play a significant role in patient outcomes.
Results
Overall:
Patients followed for 24 to 72 months. Out of 915, complete follow-up data was collected from 618 patients. (Patient attrition due to loss of follow-up, death etc. was accounted for in this study).
21 patients found to have metastasis (celiac lymph nodes) during lymph node dissection.
There was no different in the number of nodes dissected with either approach, however, there was a higher number of positive nodes in patients undergoing Ivor-Lewis with an open laparotomy. (28.7 % versus 38.7% with Ivor Lewis). Despite this finding – there was no significant different in the total number of metastasis in either approach – Sweet 42.5% and Ivor Lewis 45.2%
No difference in overall 5 year survival rate for either procedure.
Operative mortality was similar in both groups (2.3% for Sweet, Ivor Lewis 1.8%)
Sweet versus Ivor Lewis
– Shorter surgical time with Sweet approach (181 min +/-71 minutes) versus 208 minutes for Ivor Lewis (+/- 63 minutes).
– Less blood loss (and less transfusions) with Sweet approach
– Fewer complications
Overall rate of complications: Sweet 12.3%. One fifth of all Ivor Lewis (IL) patients experienced post-operative complications (20.4%)
wound infection: Sweet 3.2% IL 7.8%
delayed gastric emptying: Sweet 1.7% IL 4.7%
Anastomotic leak: Sweet 2.1% IL 4.2%
– Shorter length of stay
Average length of stay was 13.2 days for patients undergoing the Sweet procedure compared to 17.3 days for the Ivor Lewis group.
In addition, while only 4.4% of the Sweet group remained hospitalized for more than 30 days after surgery, 12.6% of the Ivor Lewis patients had a length of stay greater than 1 month.
Discussion
More positive nodes, but Why?
The increased finding of positive lymph nodes in patients undergoing the Ivor Lewis merits further discussion and investigation as to whether this is related to the areas of lymph node dissection since the authors discuss the difficulty of assessing areas of the anterior mediastinum. There is no mention of how using a single incision technique and accessing the stomach via the diaphragm affected abdominal lymph node dissection.
While the actual numbers harvested using either technique were comparable, were the surgeons able to harvest more lymph nodes from specific sites in the patients with an open laparotomy?
If so, this supports the notion that for some cancer operations, like this one, where accurate staging is absolutely essential for determining prognosis – open surgery may remain superior to “lesser” procedures such as the Sweet or minimally invasive approaches.
More importantly, the surgeons at Zhongshan illustrate both the magnitude of a surgical procedure like the Ivor Lewis and the potential benefits of alternative approaches performed by experienced surgeons.
Fewer anastomosis leaks
In their facility, patients experienced demonstrated only half the rate of wound infection with only one primary incision versus the two incision Ivor Lewis. More importantly, the incidence of a potentially lethal complication like anastomotic leak was also half (2.1%) of that for Ivor Lewis (4.2%**). While some of the literature has cited a mortality rate as low as 3.3% due to advances in the treatment of the associated sepsis, anastomotic leak remains a devastating complication.
**This rate mirrors what is seen in the literature for Ivor Lewis esophagectomies. The cited mortality for anastomotic leaks varies widely.
Limitations
The biggest limitation of this study is the retrospective design. However, at present, researchers (Dr.Haiquan Chen) at Fudan University are conducting another ongoing clinical trial to compare these procedures. This study is a prospective, randomized design.
Implications / considerations
The work done by Jua Ma et al. warrents careful reading and consideration; Zhongshan Hospital in Shanghai, China has over 1700 beds, and serves a large patient population, in which esophageal cancer is relatively common. The elevated incidence of esophageal cancer in China has been noted as far back as 2,000 years ago by Chinese scholars and physicians.

The increased incidence and presentation of patients with surgically resectable esophageal cancers combined with a robust thoracic surgery division (with over 29 thoracic surgeons on staff) provides the authors with an opportunity to collect, analyze and present data on a scale unheard of in the majority of institutions performing single-site investigation. In 2013, for example, the thoracic surgery department performed over 1152 Lung procedures and 683 esophageal procedures.
Article:
Jua Ma, Cheng Zhan, Lin Wang, Wei Juang, Yongxing Zhang, Yu Shi & Qun Wang (2014). The Sweet approach is still worthwhile in modern esophagectomy. Annals of Thoracic Surgery, 2014 [in-press].
References
Churchill ED, Sweet RH. (1942). Transthoracic resection of tumors of the esophagus and stomach. Ann Surg. 1942 Jun;115(6):897-920. Contains pdf of original article but loads slowly.
Naef, A. P. (2004). The mid-century revolution in thoracic and cardiovascular surgery, part 3. Interactive cardiovascular and thoracic surgery 3.
Sweet R. H. (1946). Subtotal esophagectomy with high intrathoracic esophagogastric anastomosis in the treatment of extensive cicatricial obliteration of the esophagus. Surg Gynecol Obstet. 1946 Oct;83:417-27.
Thank you to Dr. Qun Wang for his assistance.
