Today’s recommended read is for all of the thoracic surgeons out there that are interested in establishing their own nonintubated uniportal programs. This is a interesting article if you’ve taken a masterclass on uniportal technique, reviewed the literature around nonintubated surgery, but haven’t yet taken the next step to start performing this procedure at your hospital.
Thoracics.org has reached out to the corresponding author, Sook Sung for more information about their experiences with nonintubated uniportal VATS including some updates, but let’s review the primary article while we await a reply.
In the article, Nonintubated uniportal video-assisted thoracoscopic surgery: a single center experience, Seha Ahn et al. discuss their experiences over a six month period after initiating this technique in January 2017.
During this period, 40 patients underwent this technique. Pre-operative patient selection was important with multiple exclusionary criteria.
Exclusionary criteria for initial cases: General
Obesity (BMI greater than 30
Anticipated/ expected difficult airway
Persistant cough/ or high amount of secretions
At increased risk of gastric reflux
Exclusionary criteria: Cardiopulmonary
Expected/ anticipated to have extensive adhesions
Prior pulmonary resection
N2 stage lung cancer
Severe cardiac dysfunction (exact definition not defined)
Photo by 서울성모병원
Anesthesia and Intra-operative Monitoring
Prior to the procedure, patients received dexmedtomidine. At the time of the procedure, patients were maintained with infusions of remifentanyl and propofol.
No patients were intubated. Patients did receive supplemental oxygen by mask at a rate of 6 to 9 liters/ min. Oxygenation was monitored with botha small single nostril end-tidal CO2 monitor and pulse oxymetry. Anesthesia monitoring including a BIS monitor. General hemodynamic monitoring consisted of continuous EKG/ telemetry and serial blood pressure cuff measurements.
Surgical technique
As part of the surgical technique, the authors administered an intercostal nerve block for additional analgesia. In the majority of patients (35 of 40), intrathoracic vagal nerve blocks were also performed to reduce / prevent coughing during the procedure.
The procedure was carried out using a single 3 to 4 cm incision. The main surgical instruments used were a 10mm 30 degree scope, a harmonic scalpel and a curved suction tip catheter.
Results
General demographics
There were 40 total patients in this study, which spanned a period of six months. More than half of these patients (57.5%) were women. The mean age was 60.
The vast majority of these patients (72.5%) had lung cancer. Seven patients (17.5%) had surgery for pulmonary metastasis. The remainder of patients had surgery for either benign lung disease or pleural disease.
Procedure types
Over half of the patients underwent lobectomies (57.5%). 10 patients (25%) had wedge resections, with six patients having segmentectomies (15%) and a solo patient undergoing a pleural biopsy.
Complications
There were several intra-operative conversions. The majority of these conversions were related to anesthesia, with 3 patients requiring conversion to standard intubation. The authors are a little unclear with the reasons for this – with one sentence saying it was not related to hypoxia (with all patient sats greater than 90%). The authors then attribute the conversions to excessive respiratory movements, but then report that all three of the patients’ hypoxemia resolved with intubation. This is better explained in a later portion of the paper, but it is still a bit confusing as to whether excessive respiratory movement was a contributing cause for the reason to intubate mid-procedure.
There was only one conversion for surgical technique, which occurred after the dread pulmonary artery injury, with the authors converting to multi-port VATS. There were no conversions to open thoracotomy.
Post-operative complications
Seven total post-operative complications (17.5%)
3 patients with prolonged air leaks
2 chylothorax
1 delayed pleural effusion
1 pneumonia
Interestingly enough, outcomes based on traditional criteria, (chest tube days, and overall length of stay) were not significantly different that results published for more traditional types of thoracic procedures.
The average post-operative chest tube time was 3.2 days (range: 1-13 days)
The average hospital stay was 4.4 days (range 1 – 18 days).
There was one notable outlier listed, a patient with a prolonged airleak that resulted in a 20 day hospital stay.
Discussion
This article is note worthy of several reasons, in that the authors both describe their techniques and the initial results of the initiation of a new surgical approach (nonintubated and uniportal) in their facility. The authors are to be commended for reporting research results that show a (17.5 %) high rate of complications, which is presumably related to the learning curve of adopting a new surgical protocol.
However, this article would have been much more informative if there had been more of an in-depth discussion of the challenges involved in initiating and managing a nonintubated uniportal program, instead of a general review of the literature. While the article notes that there was a solo surgeon involved in these 40 procedures, there is little discussion of the prior experience of that surgeon or the anesthesia team(s) involved. What the surgeon previously experienced in uniportal VATS? If so, what was the level of experience?
The same goes for the anesthesiologists involved in this study, since a large portion of the procedure (ie. the nonintubated portion) as well as the highest level of conversions (to standard intubation) occurred under their guidance. A short discussion about intra-operative intubation would have been a helpful addition for readers as well, such as a discussion of the difficulties (or lack thereof) of intubating a patient after they have been secured into a lateral decubitus position.
While the traditional outcomes measures appear fairly unchanged in comparison to standard VATS with general anesthesia and intubation, what was the difference in related outcomes?
Was there a difference in/ would they anticipate a difference in (with larger numbers of patients):
Post-operative intubation? How man patients required urgent/ emergent intubation during the post-operative period?
Post-operative pneumonias and other respiratory complications? While the authors cite one post-operative pneumonia, there appear to be few other respiratory complications cited in this study.
Post-operative anesthetic complications such as hemodynamic compromise (requiring prolonged use of pressors, for example). What about post-operative nausea/ vomiting or gastric ileus?
Since nonintubated and uniportal techniques have been proposed as a alterative to standard surgery for high risk patients (patients with poor respiratory reserve/ cardiovascular disease), the presence or lack of these complications in patients (even specially selected patients) is important.
When reviewing the lack of clear-cut advantages such as shorter length of stay, were there other reasons for it, such as post-operative nursing care? Are there changes that need to be implemented/ have been implemented since this study was published that have resulted in fewer chest tube days, or a shorter overall length of stay?
In the time since this study was concluded, what have been this group’s continued experience? Have there been any unexpected outcomes or observations? What changes continue to need to be addressed?
Are there any other observations that the authors would like to share? While traditional journals have size and article length limitations, we don’t here at thoracics.org.
If you can only attend one thoracic surgery conference, shortlist VATS International.
Attendees with Dr. Marco Scarci (2nd from the left)
VATS International
VATS International (previously known as Cambridge VATS) is the brainchild of Mr. (Dr.) Marco Scarci. The Italian surgeon recently made the switch from NHS Papsworth (Cambridge) to the historic Royal London Hospital. Each year, Dr. Scarci gathers the world’s specialists on minimally invasive surgery to meet here in the United Kingdom to share knowledge and practice techniques for traditional VATS, uniportal approaches (standard and subxyphoid) and robotic surgery.
This is the third year of the conference and it’s reputation for dynamic speakers and controversy continues. With over 100 attendees, and a wide range of global participation as well as live surgery sessions and a wet lab, Dr. Scarci has had runaway success despite some last-minute challenges posed by his recent defection from the Cambridge facility. (Having met several members of the rather staid and traditional thoracic surgery department at Cambridge, Dr. Scarci, with his emphasis on minimally invasive surgery, is undoubtedly better-suited to the London-based facility).
Excellent lecture content, dynamic speakers
There were several excellent speakers, making it difficult to narrow the selections for presentation here. The obvious standout was Dr. Lim, (as discussed in a previous post).
As one of the course directors, and the inventor of the uniportal approach, Dr. Diego Gonzalez Rivas gave several lectures on the technique aspects of uniportal VATS.
Dr. David Waller followed up with a lecture entitled “Intra-operative problems in VATS lobectomy: Avoidance and Management.” He discussed complicating patient factors such extensive adhesions, anthrocotic lymph nodes, anatomical variance and incomplete fissures that increase the complexity of uniportal cases. He also identified common surgical problems such as difficulty identifying the target lesion, development of large air leaks and inadvertent damage to hilum or bronchus with strategies to prevent & manage these issues. He reviewed surgical techniques on bleeding control/ major vascular injury as well as absolute indications for surgical conversion such as equipment failures, airway injuries and stapler jams. In closure, he also warned against using conversion rate as an outcome measure. It was a fairly dry lecture despite being an interesting and important topic.
Among the remaining speakers, the overwhelming theme of change, and evolution along with an underlying sense of defiance continued. These surgeons are here to discuss, learn and practice uniportal surgery even if more traditional surgeons don’t approve.
Some of the best presentations were:
Dr. Alan Sihoe, (Hong Kong) gave a modified lecture called “Reasons not to perform uniportal VATS lobectomy”. This lecture which was adapted from a previous lecture from last year’s conference also addressed criticism of uniportal VATS. He reviewed the existing literature on uniportal surgery which suggests that uniportal surgery is a safe alternative to other surgical approaches.
Dr. Alan Sihoe
During the lecture, Dr. Sihoe encouraged surgeons to move past case reports to performing higher level research such as randomized control studies to create evidence in the area of uniportal surgery. He also encouraged participation in the European database, to gather prospective data on uniportal surgery. Until there is a larger body of literature utilizing higher levels of evidence, uniportal surgery will continue to face significant (and justifiable) criticism as a fad procedure. While it wasn’t a ground-breaking lecture by any means, it was also a reminder for thoracic surgeons to think like a researcher. It was a good follow-up on Dr. Lim’s opening lecture.
Dr. Gaetano Rocco (Italy).
Dr. Rocco, one of the pioneers of the uniportal approach, continued the discussion of the need for evolution and adaptation but with a different approach in a talk entitled, “VATS major pulmonary resection for (very) senior surgeons. He extended an olive branch to older, experienced thoracic surgeons with limited experience with VATS. His lecture discussed the ways to remediate older surgeons, and build their skills and comfort level in performing VATS procedures. His lecture offered a clear-cut and concrete , step-wise curriculum and self-assessment tool for surgeons looking to improve their VATS skills, starting with VATS lobectomy.
Dr. Gaetano Rocco (left)
Dr. Ali Khan (India) delivered two lectures, the first on operating room technology, but it was the second on uniportal surgery for inflammatory and infectious diseases that really piqued my interest. Part of this is due to my interest in the surgical treatment of tuberculosis, and my great appreciation for empyema as a surgical disease. Most readers know that reducing the time from presentation/ diagnosis of empyema to surgical decortication is one of my goals in daily practice, so any reminder that the morbidity/ mortality of decortications have been greatly reduced by minimally invasive surgery is always welcome.
Dr. Ali Khan
Honorable mention: Dr. Alex Brunelli, “Fast track enhanced recovery for MITS”. Basically a talk on care plans with specific markers for timely progression and discharge. While this is standard fare for nurses, the use of care plans for many surgeons is unfamiliar territory. It would have been nice if the care plans were available as a handout for surgeons who are still fine-tuning their own programs. It also would have been nice for a better breakdown of how specific items reduced the length of stay (how/ how much) or decreased the rate of complications. Nice to mention care plans but better to have measurable and specific examples.
After the extensive lecture series on the first day of the conference, the second day was devoted to live surgery cases and the practice lab.
Wet Lab
Since animal research of any kind is tightly controlled in the United Kingdom, 3D printed models were used for the wet lab portion of the course.
3D model of thoracic cavity
This is the first time that this type of model has been used. While the green plastic housing looks rudimentary, on closer inspection of the ’tissue’ inside, one gets a better appreciation for the models. The tissue is soft, and sponge-like. The lung doesn’t inflate but appears more lifelike than other models.
I don’t have the patience or temperament to shoot video footage, but I did record a couple of seconds so readers could have an idea what the wet lab portion of the course is like. In the video, Dr. Sihoe is instructing two trainees on the proper technique.
Despite its relative youth, VATS International remains one of the best conferences on minimally invasive surgery, inferior to none. This conference is highly recommended and considered superior to many of the traditional conferences on the topic (such as the annual Duke conference), due to lecture content on timely topics and controversial issues. The hands-on wet lab and participation by internationally recognized and globally diverse speakers makes this conference more valuable to attendees looking for exposure to newer surgical techniques.
Thoracics.org 2017 wish list
What would I like to see next year? As mentioned above, VATS International is one of the better courses available for surgeons interested in uniportal, subxyphoid and other minimally invasive techniques. But there is still more content I’d like to see – on nonintubated and awake surgery, for example.
However, with regards for this year’s speaker, an anesthesiologist from Papsworth Hospital, this topic would be better covered by one of the “masters” of the field; Dr. Eugene Pompeo of the Awake Surgical Group or Drs. Hung & Chen. The “Papsworth Experience” per se is limited to heavy sedation/ general anesthesia without mechanical ventilation. Patients still have LMAs and are heavily sedated. One of the main benefits of nonintubated anesthesia is the ability to operate on the medically fragile. It would be enlightening to hear more about operating on this population from more experienced clinicians. One of the topics that has been essentially ignored in the literature on this topic, is the implications for thoracic surgeons, anesthesiologists, operating room and recovery room staff on operating on this population of sicker patients. I think readers would like to hear about the new challenges in managing patients that were previously inoperable due to serious co-morbidities.
A discussion on developing or actualizing a formal certification process with examination for minimally invasive surgery with suggested curriculum, and case log requirements would be a nice addition. Blackmon et al. published a credentialing guideline but it’s a multi-part overly complex document full of “levels” of competency. I’d like to see a discussion on the development of an actual certification to be offered by a surgical licensing body or surgical society. Since the American agencies would probably take another 20 years to consider the idea, perhaps one of the guest speakers’ native society would be more willing to take on this project?
I’d also like to see at least a limited amount of content on esophageal surgery. I know, I know..While practice areas for thoracic surgeons vary around the globe, with the rapid rise in esophageal cancer, a lecture on the role of minimally invasive surgical techniques for esophageal surgery would be a great addition to the current roster of topics, particularly if it was given by one of the modern masters of esophageal surgery like Dr. Benny Weksler or Dr. Roy Chen.
Lastly, one of the most enjoyable aspects of this conference is the truly international flavor. Watching a surgeon from Israel demonstrate uniportal techniques from a practice site in Shanghai brings home the importance of global collaboration. Hearing surgeons from India, Brazil, France and Canada present data on their practices is critical to gain perspective, and exchange ideas. It also helps prevent attendees from falling into the trap of “we’ve always done it this way.” This concept could be expanded to include designated global snapshots, to highlight research or data in specific geographic areas, like Dr. Khan’s lecture on uniportal approaches for infectious and inflammatory disease.
A full lecture on cost containment techniques for surgeons practicing in hardship areas would be a great topic. Dr. Sihoe touched on the issue during one of his lectures, but since I’ve heard other surgeons talk about the limitations posed by having only one thoracoscope, I’d love to see an equipment representative give a lecture on maintaining thoracoscopes, where to donate old scopes or how to rehab these scopes for a second life. A talk about modifying existing surgical instruments for surgeons who can’t afford the Scanlan set would be helpful as well. One of the reasons these courses have been so successful it the fact that they are technically based, so adding a section like this might help spread the uniportal technique to a whole socio-economic and geographic segment of patients that it might not otherwise reach.
This last item might be a tall order for Dr. Scarci and his group but he’s done pretty well thus far.
Day One of the VATS Peru 2016 Conference was a primer for surgeons interested in learned and performing uniportal VATS. Dr. Gonzalez Rivas’ lectures formed the basis of theory and principles of uniportal thoracoscopic surgery, with additional lectures by Dr. William Guido, Dr. Timothy Young and Dr. Deping Zhao.
Surprisingly, many of the surgeons at the event informed me that they already use some uniportal techniques in their practice. But they came here to Cusco, Peru to learn more from the Master of Uniportal surgery himself, Dr. Diego Gonzalez Rivas before attempting more complicated and complex surgical cases like sleeve resections. Others came to learn more about nonintubated surgery in their uniportal patients. The remainders were the core group of surgeons who came to get their first taste of uniportal surgery.
Some came from the local areas; from Lima, from Chile, and Ecuador. Others came from other parts of Latin America; from Mexico and Costa Rico. There was even a practicing surgeon from the United States, who realized that if he wanted to pursue the most advanced surgical techniques and minimally invasive surgery in thoracic surgery, that he couldn’t do it at home. That’s a big paradigm shift for a surgeon from a nation that tends to think if it wasn’t invented in the United States, that it doesn’t exist, or has no merit. It is also, from my perspective, a welcome change.
With Dr. Tim Young, Dr. Diego Gonzalez Rivas and Dr. William Guido
In the five years that I have been travelling the globe, writing about surgical innovation, I am usually alone in my quest, in seeking innovation outside of American medicine. That’s not to say we(Americans) don’t have our own great surgeons – I can easily rattle off quite a few – but it’s an acknowledgment that surgical innovation (or any innovation in general) is not the exclusive domain of the United States. That sounds like a fairly basic principle, but one that is rarely seen in practice. American doctors and nurses just don’t attend international events to learn. They only attend to teach – and often leave as soon as their lecture is complete, ensuring that an accidental opportunity to be exposed to new ideas is minimized.
So it was a pleasure to meet the surgeon from California, who took time off from a perfectly successful practice performing routine thoracotomies, to learn more about uniportal surgery at this and another upcoming master course.
VATS Peru 2016 – learn uniportal and subxiphoid techniques in the wet lab, at the hands of the inventors of these techniques at this year’s conference in Cusco, Peru.
Cusco, Peru – September 2016
The 2016 VATS Peru conference and wet lab is scheduled for September 7th – 9th and this year’s agenda looks to be interesting and exciting.
Dr. Carlos Fernandez Cristoso is this year’s director of the course, and he has all the essentials of uniportal (single port thoracic surgery) VATS including special sections on : Management of intraoperative bleeding, difficult / advanced uniportal cases, and uniportal VATS on awake and nonintubated patients in addition to much of the standard uniportal fare.
Dr. Diego Gonzalez Rivas is honorary president of the course.
The course also includes lectures on the uniportal subxiphoid approach, as well as how to teach uniportal approaches to residents and fellows. The surgeons of Shanghai Pulmonary Hospital as well as Dr. Diego Gonzalez Rivas , the inventors of subxiphoid and uniportal approaches (respectively) will be there. The surgeons of Shanghai Pulmonary Hospital will be sharing their experiences of performing over 8000 uniportal resections a year, as well as presenting a live case direct from Shanghai during the conference.
Also – this conference is unique in offering an opportunity for surgical assistants, and scrub nurses to gain insight and share experiences in uniportal techniques with concurrent courses scheduled for operating room nurses. Both sections spend the last day of the conference in the wet lab applying newly learned techniques.
To register for this course – click here or e-mail : consultas@vatsperu.org
Dr. Ming-Hui Hung & Dr. Jin-Shing Chen at National Taiwan University Hospital talk about their work in nonintubated and awake thoracic surgery.
After attending multiple recent thoracic surgery conferences, where the topic of nonintubated thoracic surgery sparked murmurs and outspoken criticism, thoracics.org conducted a brief review of the literature to attempt to discern if this criticism and skepticism was warranted. As part of this review, we reached out to several of the leaders in the field, including Dr. Ming-Hui Hung, a well-respected Taiwanese anesthesiologist and widely acknowledged expert on this topic.
Thoracics.org asked for Dr. Hung’s commentary as well as his response to several specific questions on nonintubated thoracic surgery. Here is his response in it’s entirety (re-formatted to fit the Question and Answer format posed by our correspondence).
Question: Would you tell me more about your initial research in this area. What lessons have you learned (overall) in patient selection for non-intubated thoracic surgery? What additional tips or advice would you offer interested thoracic surgeons/ members of anesthesia?
As we had discussed in our publications, we are facing more and more aging and frail patients with minor thoracic procedures. As surgical approach evolves toward a minimally invasive thoracoscopic technique, we expect that there would be a need for less invasive anesthetic management (i.e. nonintubated VATS) as well. Traditional intubated one-lung ventilation does offer a safe and quiet surgical environment for surgery; however, we still suffer occasionally to have patients complicated with intubation-related adverse effects, not to mention the consuming procedures for successful one-lung ventilation. Actually, there was a short-stature elderly lady complicated with pneumo-mediastinum because of tracheobronchial laceration after a double-lumen tracheal intubation. We was driven by this case we suffered to find a solution and whereas we developed our nonintubated techniques since 2009. As you noted, now nonintubated VATS is a routine part of our armamentarium for thoracic surgery.
To summarize, there are important steps that we learned from our experiences:
Thoracic epidural anesthesia (TEA) vs internal intercostal nerve blocks (INB)
In the beginning, we applied TEA. It does provide satisfying analgesia but it is time-consuming and carries more risks for neurological complications. Once again, we had a nonintubated case coincidentally complicated with acute transverse myelitis after surgery. Although we excluded the epidural procedure per se, to be the direct cause of the regretful complication, we were still bothered by a legal suit against us. Then we learned that internal INB is equally effective as a thoracic epidural catheter. It saves time and risk free to do it as we do it under a direct vision by scope, and no touching on any spinal structures. Now INB is our routine part of nonintubated VATS. TEA is considered for those doing a bilateral VATS. We think this is important because it makes nonintubated VATS more safe and even more less invasive, for which our patients would accept this approach more. We Taiwanese are mostly reluctant to have someone doing anything on our spines, as we usually call them the “dragon bones”, the most important part of our bodies.
Intrathoracic vagal block
Since cough reflex is a visceral part of autonomic nerve, which is not blocked by TEA or INB, unpredictable cough reflex during surgery could quietly bothering and even dangerous. We soon learned that we could block the cough reflex via intrathoracic vagal nerves. It really works. It alleviates the tension upon surgeons who working on a spontaneously breathing lung and enable them more manipularity of lung parenchyma and hilar structures. Surgeons are still needed to be as gentle as possible for that excessive traction still can trigger cough reflex from the dependent side where vagal nerve function is intact.
Sedation and titration of its depth
We know there is an “awake, or not awake” issue on nonintubated VATS. We prefer to sedate our patients just because our patients do not want to be awake during surgery. Lateral decubitus position is not a confortable position. Most of our patients undergo surgery because of lung cancer or potential lung cancer. It usually takes 1-2 hours to have a diagnosis first and complete the definite treatment upon the final pathological result. We believe no one would like to be anxiously awake for the result with an open chest in an awkward position. In addition, the initial phase of iatrogenic pneumothorax would cause the patient dyspneic and tachypneic for a while, giving patient sedated with supplemental opioid is useful to alleviate the respiratory disturbances and accelerate the operated lung to collapse. By applying bispectral index EEG monitor, we can observe the BIS index increasing during the initial phase of open pneumothorax, it could be caused by inadequate analgesia, or just because of a dyspneic response. We may give the patients some more anesthetic and it usually recovered after effective vagal block. Carefully observe the respiratory pattern (from the video, or using an noninvasive end-tidal capnography) is of importance. Anesthesiologists should keep vigilant on the respiratory pattern and airway patency of the nonintubated patients, including a plan B for intubation conversion.
Patient selection
We operate on spontaneous breathing lungs (most of the time, the operated lung collapses well because of positive pressure introduced into the chest cavity). The remaining opposite lung is sufficient to maintain satisfactory oxygen saturation, despite unavoidable hypoventilation. However, a vigorous diaphragm would jeopardize the balance. For surgery, it causes excessive movement of the operated lung and makes hilar manipulation dangerous or even impossible. For respiration, CO2 rebreathing (an to-and-fro phenomenon between the dependent and the non-dependent lung) would further exacerbate the breathing pattern and decrease the alveolar oxygen fraction of the nondependent lung, leading to oxygenation desaturation. It is the most common scenario of our difficult cases and we changed to intubation conversion in some of them, especially in major resections (i.e. lobectomy) for lung cancer. We learned that obese patients tend to be an abdominal breather because of an elevated diaphragm and they are usually associated with excessive diaphragmatic movement during nonintubated surgery. Other contraindications for nonintubated VATS are also listed on the literature. We suggest that are mostly at the discretions of the caring surgeon and anesthesiologist as their good clinical practice routines.
Question: How have your findings of your work been received internationally? At several recent conferences, there has been a lukewarm or even critical response towards nonintubated thoracic surgery. Is this a frequent response?
A typical unfriendly tone from other colleagues is “just because it can be done, should it be done?” We have the same feelings as you experienced in those meeting. Nonetheless, our findings are relevant and robust that nonintubated VATS is feasible and safe in selected patients with a variety of thoracic procedures. They were published in well-known surgical journals in cardiothoracic field, including Annals of Surgery, Journal of Thoracic and Cardiovascular Surgery, Annals of Thoracic Surgery and the European Journal of Cardio-Thoracic Surgery. Still, there are surgeons and anesthesiologists enthusiastic about less invasive alternative for their caring patients visiting our hospital for nonintubated VATS, including Korea, China, Switzerland internationally and other hospitals nationally.
We believe it is human nature being anxious and doubtful to do something you do not get familiar with, especially when intubated one-lung ventilation is nearly an unbreakable only golden standard for thoracic surgery for decades, and almost all thoracic surgeons in current generations would request a fully collapsed lung to operate upon. But at this time, we are approaching a 1000 nonintubated VATS case volume, and all thoracic anesthesiologists and thoracic surgeons in our hospital are dealing with nonintubated VATS if this is appropriate for their patients. We think it is quiet a milestone in our program.
Five years ago, I asked one of my colleagues, a nursing anesthetist [emphasis mine] whether she would choose nonintubated technique if she needs a VATS procedure.
She said, “Well, I need to think about it. You better give me an double lumen even though I know how big it is.”
One year later, her answer to the same question is a “Yes, please, no tube.”
Question: Are there any other obstacles for researchers in this area? Do you have other on-going research programs at your facility?
Obviously, nonintubated patients recover from surgery fast. They can shift to the gurney on their own from the surgical table. They experience less pain and less PONV in PACU, which enables them to recover oral intake sooner with oral analgesics and early ambulation, not to mention those common adverse effects after double lumen intubations, such as a sore throat and a change of voice quality. Currently, we are drafting our manuscripts about nonintubated VATS pulmonary resection in patients with compromised lung function. Meanwhile, a randomized trial is under investigation to compare the recovery differences of nonintubated VATS vs. intubated VATS. There are also several more nonintubated trials in Clinicaltrial.org in different countries.
Question: Do you know of any programs that have adopted your techniques and protocols?
To our knowledge, Dr. Jianxing He from the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, China, is also an enthusiastic advocator and pioneer in nonintubated VATS. He is also leading journals such as Journal of Thoracic Disease andAnnals of Translational Medicine as an open forum to accelerate the impact of nonintubated VATS. He is going to publish a state-of-the-art monograph dedicated to nonintubated VATS in the near future. We believe you can get useful information regarding nonintubated VATS in China and different perspectives from him.
As always, we keep doing our best to satisfy our patients’ need during their curing and recovery processes, just because “our patients, first.”
Ming-Hui Hung, MD, MS
Anesthesiologist, Department of Anesthesiology
Jin-Shing Chen, MD, PhD
Professor, Department of Surgery
National Taiwan University Hospital
Thoracics.org would like to thank Dr. Hung and his colleagues for their continued work in this area. Thoracics.org would also like to thank Dr. Hung for his willingness and frank candor in addressing some of the other issues in this area.
Readers: Thoracics.org has highlighted a key phrase in Dr. Hung’s response that also, unintentionally but directly addresses one of the criticisms recently advanced by a noted American thoracic surgeon who challenged Dr. Martinez as to whether he would ever delegate the care of a nonintubated patient to a nurse anesthetist. When Dr. Martinez hesitated in his response, the surgeon claimed victory, stating, “See? That would never work in American hospitals, [where certified nurse anesthetists oversee the majority of cases]”. This was his rationale for dismissing this technique, even when it might make otherwise inoperable patients eligible for life-saving surgery. That dismissal of both his American colleagues and the needs of the more fragile subset of our thoracic surgery population demonstrates some of the limitations in our so-called “masters” or “giants” of thoracic surgery. While great, and influential surgeons, they are not infallible. Their experiences carry wisdom, but their opinions shouldn’t carry more weight than any other published study.
Thoracics.org is committed to giving a voice and forum to all specialties and members of the thoracic surgery community.
the second annual Cambridge VATS : uniportal VATS, nonintubated thoracic surgery and the masters
Cambridge, UK
Cambridge center for continuing education
It may only be the second annual Cambridge VATS conference but Dr. Marco Scarci has managed to assemble one of the finest assortments of speakers in one short course since the days of the original giants. This included a roster of the biggest names, publishers of innovative research and the Masters of Minimally Invasive Surgery including Gaetano Rocco, Alan Sihoe, Joel Dunning, Thomas D’Amico, Henrik Hanson and Diego Gonzalez Rivas.
Dr. Ismail (Berlin), Dr. Hansen (Copenhagen) and Dr. Alan Sihoe (Hong Kong)
However, one of the standout presentations was given by none other than Dr. Guillermo Martinez, an Argentine anesthesiologist from Cambridge’s own Papworth hospital. He immediately leapt into one of thoracic surgery’s more controversial topics, nonintubated thoracic surgery. While Dr. Martinez primarily focused on the nonintubated but heavily sedated (or generally anesthetized patient with LMA for airway support) he gave an excellent presentation on the anesthetic considerations for nonintubated surgery. As he explained, it’s a natural progression for nonintubated surgery and VATS go hand in hand, as surgeries become less traumatic to patients, the anesthesia should be less invasive as well. He discussed the rationale for nonintubated surgery from an anesthesiologist’s perspective and outlined the practices at Papworth Hospital where he is part of the thoracic surgery team.
He also discussed the many challenges posed by this method of patient management including the fact that anesthetic techniques for nonintubated surgery need to be reproducible, safe and feasible for eligible patients. Anesthesiologists and thoracic surgeons also need to pre-establish criteria for conversion (such as heavy bleeding, patient hemodynamic instability or conversion to open surgery) to general anesthesia prior to cases, and to be fully prepared to perform urgent intubation as needed.
He also touched on the methods of analgesia used during these cases such as adjuvant like local anesthesia (chest wall infiltration), regional blocks and thoracic epidurals as well as cough suppressant mechanisms.
Reigniting controversey
This along with Dr. Diego Gonzalez Rivas’ subsequent presentation on uniportal surgery combined with nonintubated and awake thoracic surgery reignited much of the firestorm that we first saw at the Duke conference.
Dr. Diego Gonzalez Rivas
Commentary by Dr. Eric Lim perfectly captured some of the sentiments of younger members of the audience, when he took the stage as part of a separate debate on the merits of VATS versus SART when he stated, “I am tired of surgeons calling [new techniques/ technologies / treatments] crap when they’ve read the papers and seen the videos [demonstrating the procedure]. It’s not crap – if you just watched it.” He continued to address the resistance to change in surgery, and the attitudes of surgeons unwilling to adapt. It was a refreshing moment of forthrightness and candor that has been sorely missing from many events. It was also a 180 degree perspective from many of the more critical and conservative attitudes that liken techniques like nonintubated, awake anesthesia or uniportal surgery as being a type of showmanship rather than real innovation, or critics who question the relevancy of pursing research in this area with the “just because we can do it, should we?” mantra that has pervaded many of the recent surgical discussions.
Representatives from Shanghai Pulmonary Hospital (SPH) also gave several presentations. Dr. Haifeng Wang discussed high volume surgical training while Dr. Lei Jiang discussed uniportal surgery using a subxyphoid approach.
Dr. Wang explained how the research and lessons learned from the Shanghai Pulmonary Hospital has authenticated the uniportal VATS technique to many surgeons in China. He presented original data from his facility on over 1500 uniportal cases.
While he and his colleagues initially debated the safety of this procedure, after learning this technique, it has been adopted throughout Shanghai Pulmonary Hospital. He and the 39 other surgeons on staff use this technique every single day. In fact, the sheer volume of cases at Shanghai Pulmonary Hospital has made these surgeons some of the most experienced uniportal surgeons in the world. After the first uniportal VATS case was performed at SPH in 2013, the technique has rapidly gained popularity. Last year (2014), surgeons at SPH performed 6855 cases, with uniportal cases comprising 50% of all cases. That percentage will only grow, as this year, the hospital is on target for over 8000 cases.
Cambridge 2016?
Now, with such a great entree, what will be the encore for 2016? It would be great to see more “micro-invasive surgery” like a serious sit-down debate among the Awake Thoracic Surgical Group, Gonzalez Rivas, Hung et. al and the traditionalists on the merits of nonintubated surgery along with presentation of more original research, on-going projects and a meta-analysis of the work to date in this area.
It would be interesting to hear more from Dr. Scarci himself, who has been responsible for bringing these surgical innovations to the NHS specialty hospital in Cambridge. Like Dr. Alan Sihoe, who spoke during this session on how to start a uniportal program, Dr. Scarci himself undoubtedly has some excellent experience and insights to share.
More subxyphoid, including bilateral surgical case presentation or a live surgical case also top the wish list here at Thoracics.org.
That doesn’t mean that all of the old standards should be phased out – Henrik Hanson’s standardized approach to 3 port VATS is a classic, for good reason. As Dr. Hansen said himself, “The Gold Standard should not be what Diego [Gonzalez Rivas] or I can do, but a safe, standardized approach.” Not every surgeon is ready to embrace subxyphoid or uniportal approaches, and particularly for surgeons in the twilight of their careers, maybe they shouldn’t. But there is certainly no excuse for any thoracic surgeon on the planet not to excel at traditional VATS.
Topics that should be retired include debates on whether VATS of any approach respects oncological principles, and many of the topics in Robotic surgery. If it’s anyone but Dr. Robert Cerfolio or Dr. Mark Dylewski, then there’s probably not much that they can add to the topic. For everyone else, robotic surgery remains more of an expensive surgical toy than a legitimate area of research. In that vein, less presentations on developing toys and more guidance to the younger audience on transitioning from case reports to more academic research would make for a nice change. If we are going to continue to promote minimally invasive surgery, that we should encourage more advanced research; like the development of more randomized or multi-site trials on topics in this area.
Single port thoracoscopic surgery and awake anesthesia: the micro-invasive thoracic surgery? The current research and use of these state of the art techniques to bring minimally invasive surgery to complex surgery and high risk patients.
At a recent high-profile American thoracic surgery conference, one of the speakers presented data from his program showing the safe and effective use of regional and conscious sedation techniques to perform complex thoracic surgery procedures on non-intubated patients.
Instead of being greeted with enthusiasm or professional interest, the great majority of well-known giants in thoracic surgery dismissed the idea with a few, repeated sarcastic, albeit joking remarks about the inconvenience of having conscious patients in the operating room. This attitude seemed perplexing given the results of Pompeo et; al.’s (2014) survey of the European Society of Thoracic Surgeons, in which a large number of respondents (59%) reported using nonintubated thoracic surgery (NITS) procedures. These mixed attitudes led thoracics.org to perform an in-depth literature search to determine the state of non-intubated thoracic surgery.
What is the current status of non-intubated thoracic surgery (and the literature surrounding it)?
Is it a wild, unsustainable idea promoted by a few dynamic but misguided surgeons? Is it a well-researched and promising developing technique that is being rejected by surgeons who may lack vision? Or does it fall into that gray area where we suspect that this technique has real value and benefits for a special subset of patients but there isn’t quite enough high level clinical evidence to demonstrate that to the surgical community?
Is non-intubated thoracic surgery destined to fall to the same fate of VATS – a game-changing technique that emerged in the early 1990’s, has been clinically demonstrated to be superior to open surgery with an overwhelming preponderance of evidence, but still being discussed by many surgeons as the ‘new kid on the block’**? Will people still debate the merits of non-intubated surgery ad infinitude thirty years from now, even when clinical guidelines have made it the standard of care (like VATS and oncology surgery)? Will there be the same reluctance to set firm standards for training in these techniques?
“Not a new concept”
photo courtesy of the US Army
As it turns out – non-intubated thoracic surgery is not a new idea or concept. It was developed early in the 20th century and was used successfully for many years for even the most complex thoracic cases such as esophagectomies until the development of double lumen intubation in the 1950’s made the use of single lung ventilation possible (Gonzalez-Rivas et. al. 2015, Pompeo 2015, Kiss & Castillo 2015). Since its rediscovery in the last several years, many of the problems that plagued this technique during its inception over a century ago have been addressed through better understanding of human physiology. Now, this seemingly fringe technique has been shown to be a feasible approach for treating the very margins of the thoracic surgery population (the extreme elderly, patients with advanced respiratory disease or other serious medical co-morbidities) that are often deemed inoperable using current techniques.
The dreaded complication (spontaneous pneumothorax) of early use of this technique by pioneers in thoracic surgery has now become one of the main advantages. Surgically created pneumothorax results in almost perfect deflation of the operative lung, achieving better results than even the most experienced of anesthesiologists using traditional single lung ventilation. Surprisingly to many observers, instead of creating a ventilatory emergency, this process is readily tolerated by most patients, even those with poor baseline pulmonary function (David, Pompeo, Fabbi & Dauri, 2015).
Current research
The majority of the current series of research on this topic are being performed by a small group of surgeons which includes Dr. Diego Gonzalez Rivas (Spain), Dr. Eugenio Pompeo and the Awake Thoracic Surgery Research Group in Italy and Dr. Ming-Hui Hung and colleagues (Taiwan). Pompeo’s group (Drs Benedetto Cristino, Augusto Orlandi, Umberto Tarantino, Tiziana Frittelli (General Director of the Policlinico Tor Vergata), Leonardo Palombi, Paola Rogliani, Roberto Massa, Mario Dauri) has been especially prolific in 2015 after several of their works were published in a special issue of Annals of Translational Medicine.
In multiple studies, these researchers have reported successful thoracic surgery outcomes in non-intubated patients, thus eliminating the majority of risks related to general anesthesia as well as uni-lung ventilation via mechanical ventilation and intubation. In several of these studies, the authors were also able to successfully perform these surgeries in fully awake patients (versus consciously sedated), making surgery possible for even the frailest of candidates. These studies included a small number of comparisons between traditional and non-intubated surgeries. While the numbers of patients enrolled have been small, and there are few randomized studies, the results have been encouraging.
Chen et. al
Chen et. al’s 2012 study has been one of the largest studies to date, with 285 cases. In this study, patients underwent lobectomies, wedge resections and segmentectomies with 4.9% requiring conversion with tracheal intubation. Lung resection was undertaken with traditional (3 port) VATS or a needlescopic approach.
The authors report the biggest problem they encountered was increased bronchial tone and airway hyper-reactivity during manipulation of the pulmonary hilum during lobectomies and segmentectomies. This was effectively treated without significant alteration in hemodynamics via intrathoracic vagal blockage which eliminated the cough reflex in these patients.
The authors caution judicious patient selection to prevent emergent conversion (intubation) particularly while surgeons are initially attempting this technique. Chen et al. also believe that non-intubated thoracic surgery is best suited for petite or small-sized female patients because the small tracheal size of these patients predisposes them to a higher rate of complications and potential tracheal injury with traditional surgery and intubation.
Awake anesthesia and lung volume reduction surgery
Pompeo et. al’s review of the literature surrounding of the use of this technique in patients with severe emphysema undergoing nonresectional lung volume reduction surgery (LVRS by awake anesthesia) showed significant treatment advantages for patients undergoing lung volume reduction surgery without intubation or administration of general anesthesia.
With an average mortality of 5% and a morbidity of 59% for traditional lung volume reduction surgery as reported during the National Emphysema Treatment Trial, findings from Tacconi et al.’s 2009 study of 66 LVRS awake patients (matched with 66 patients undergoing traditional surgery) appears promising. The authors report a reduced incidence of prolonged air leaks (18%) versus 40% in the traditional surgical group as well as a decreased length of stay. In this study, 3 patients required conversion to general anesthesia – one patient due to an elevated paCo2 of 83% and the remaining two patients for anxiety attacks.
Rate of intubation/ respiratory failure/ mortality in Tacconi et al.
Mortality in both non-intubated and the traditional surgical group was the same, with one patient from each group. In both cases, the patients had developed massive airleaks following surgery. In the non-intubated group, the patient developed acute lung injury requiring intubation of POD#12 and died POD#38.
In the traditional surgical group, 4 patients were unable to be extubated at the end of the case, with one patient requiring an additional day of mechanical ventilation. Another patient was reintubated on POD#3 for respiratory failure and died on POD#67.
Pompeo et. al, over the course of over eleven years, have also investigated the use of non-intubated (and awake) thoracic surgery for a wide variety of cases including urgent /emergent cases, wedge resections, decortications, talc pleurodesis as well as nonintubated anesthesia combined with single (uniportal) thoracoscopic approaches (aka “microinvasive thoracic surgery”).
Anesthesia for non-intubated thoracic surgery
The role of anesthesiologists in caring for patients undergoing non-intubated or awake thoracic surgery is more challenging than general anesthesia. While thoracic anesthesia already requires specialized skills for initiating, managing and maintaining uni-lung ventilation, the switch to non-intubated patients with either localized anesthesia or conscious sedation adds a new set of complexity to managing these often frail patients. Kiss & Castillo (2015) in their review of the literature, provide an excellent overview of the pros and cons of non-intubated anesthesia as well as guidelines for patient selection and eligibility criteria for use of this technique. Special populations who may benefit from this technique include patients with severe respiratory disease (and a high risk of ventilator dependency with intubation), patients with severe but stable dyspnea, or multiple cardiovascular and respiratory co-morbidities.
Kiss et. al also reviews the contraindications to use of this technique including: phrenic nerve paralysis on the non-operative side, patients at risk for difficult intubation, or patients who are unwilling to undergo awake thoracic surgery. Wang & Ge (2014) expand on these complications to include ASA status 4 or higher, bleeding disorders, decompensated heart failure, extreme obesity, unfavorable airway or spinal anatomy as well as specific respiratory conditions including bronchiestasis, asthma, sleep apnea, clinically significant sputum production and strict contralateral lung isolation.
Wang & Ge also give specific anesthesia dosing guidelines for conscious sedation, local anesthesia and regional blocks in additional to monitoring parameters.
Alterations in oxygenation and ventilation
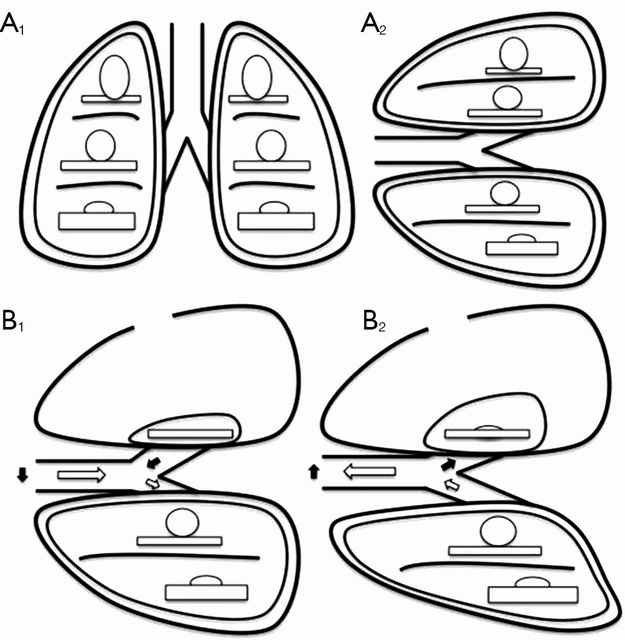
David et. al. (2015) describe the pathophysiology and alterations in oxygenation and ventilation in surgical pneumothorax including hypercapnia, hypoxia and the associated hypoxic pulmonary vasoconstriction that occurs along with the development of intrapulmonary shunt as the deflated (and unventilated lung) maintains perfusion. The authors also explain how this effect can be either exacerbated or minimized thru the choice of anesthetic agents, and the administration of supplemental oxygen, which further demonstrates the importance of involving the thoracic anesthesia team in preparation for non-intubated cases.
The relationship between ventilation and perfusion. (A) Relationship between ventilation (roundes) and perfusion (rectangles) in different lung zones, in upright (A1) and lateral position (A2); (B) relationship between ventilation (roundes) and perfusion (rectangles) in lateral position with surgical pneumothorax, during spontaneous inspiration (B1) and exhalation phase (B2). Black arrows show paradoxical ventilation and mediastinal shift. (Illustration and caption from David et. al, 2015)
This “permissive hypercapnia” has been reported in multiple articles as having minimal to no clinical effects and is easily treated with supplemental oxygen by nasal cannula or facemask.
Editor’s note: In advance of this article, Dr. Pompeo, Dr. Gonzalez Rivas and Dr. Min-Hui Hung were contacted for their additional comments and insights on non-intubated thoracic surgery. This and subsequent articles may be augmented, as applicable with their replies.
Conclusion
Should we really abandon pursuit of better patient outcomes, faster mobility, recovery and reduced length of stay in lieu of the security to tell off-color jokes with our patients safely under general anesthesia? Should we abandon all hope in treating patients previously deemed inoperable due to our own fears and hesitations to embrace newer techniques and procedures?
Or as Mineo et al, suggests, should we enlist our colleagues to design and devise several large scale studies at multiple institutions so that we can move to the next level of investigation and answer the question: “Should my patient be awake for this?”
Mineo TC, Tacconi F. (2014). Nonintubatedthoracic surgery: a lead role or just a walk on part?Chin J Cancer Res. 2014 Oct;26(5):507-10. doi: 10.3978/j.issn.1000-9604.2014.08.11. No abstract available. Very enjoyable, almost conversational article with the authors sharing their experiences with non-intubated thoracic surgery while calling for larger clinical research studies on the topic.
Pompeo, E. (2015). Non-intubated thoracic surgery: nostalgic or reasonable? Annals of Translational Medicine, 2015; 3(8): 99. Review of the historical development on non-intubated thoracic surgery and techniques in regional anesthesia for complicated thoracic surgery procedures including esophagectomies in the era predating the development of double lumen intubated and unilung ventilation. A timely reminder that some of the greatest developments in medicine and surgery are ‘rediscoveries’ of our predecessors.
Pompeo E; Awake Thoracic Surgery Research Group (2012). To be awake, or not to be awake, that is the question. J Thorac Cardiovasc Surg. 2012 Jul;144(1):281-2; author reply 282. doi: 10.1016/j.jtcvs.2012.01.083. No abstract available. Comment on article by Noda et. al.
Note: This is not an exhaustive list of literature available on this topic but a select listing of the most recent and relevant citations (and are available as free full text).
**Long time readers of thoracics.org may have noticed that we no long cover or report on ‘debates’ or discussions as to whether VATS can be used in oncology cases, or whether an adequate lymph node dissection can be performed using VATS. The literature clearly demonstrates that it can – and clinical guidelines reflect this, making the discussion one-sided, tedious, out-dated and repetitious.
Dr. Diego Gonzalez Rivas discusses intubated and nonintubated uniportal thoracic surgery for complex thoracic procedures
Orlando, Florida
Dr. Diego Gonzalez Rivas discusses non-intubated thoracic surgery
One of the standout presentations on Day One of the Duke Masters of Minimally Invasive Thoracic Surgery was Dr. Diego Gonzalez Rivas’ presentation on performing uniportal surgery on non-intubated patients. Surprisingly, this presentation was greeted with significant skepticism in the form of comments by fellow presenters.
No trocars, no rib spreading, one incision (with no rigid port placement)
The use of one small 2.5 cm incision with the camera placed above the instruments allows the surgeon to maintain the traditional perspective of open surgery using a minimally invasive approach. “Eyes above hands” Dr. Gonzalez states, reminding surgeons how to keep their visual perspective unaltered. He also discussed some of the findings from an upcoming 2016 paper [in-press] entitled, “Pushing the envelope” which reviews the developments in the areas of single port (uniportal) thoracic surgery in non-intubated patients. This along with his new textbook, have dominated the international thoracic surgery news in recent years.
As part of his discussion, he demonstrated the ease and feasibility of performing a complete and thorough lymph node dissection using the uniportal approach.
Complete paratracheal lymph node dissection in a non-intubated patient
He also presented several complex thoracic cases such as a bronchial sleeve resection for carcinoid tumor in a young, otherwise healthy female, as well as a double sleeve case, and a uniportal bronchovascular reconstruction. He discussed distal tracheal resection using high frequency ventilation jet in a non-intubated patient after resecting the carina – tracheal anastamosis and several chest wall resection cases via the uniportal approach. But the main portion of his talk was devoted to the specifics of non-intubated surgery – from anesthesia protocols to creating a anatomic (surgical) pneumothorax which eliminates problems of lung inflation during surgery. He discussed that while totally awake nonintubated surgery can be performed (with patients awake and talking), that he prefers the use of conscious sedation for patient comfort.
Nonintubated patient – VATS lobectomy
He highlighted the benefits of these approaches – with non-intubated surgical techniques allowing surgeons to operate on frailer, sicker patients who might otherwise be ineligible for surgery. He also talked about the benefits of uniportal surgery versus robotic surgery. Uniportal surgery is faster, and cheaper than costly robotic techniques that require lengthy patient positioning as well as the use of robotic tools that have to be replaced after 10 to 20 cases.
He also reviewed the relative contraindications for nonintubated surgery:
obese patients (BMI greater than 35)
patients with Malpati scores of 3 or 4 (difficult to intubate patients – in case of the need for emergent intubation)
patients with pulmonary hypertension (who will not tolerate permissive hypercapnia)
Masses greater than 6 cm in size
But he also reminded attendees that relative contraindications often change in the face of more experience.
Highlights from Day One of the Duke Masters of Minimally Invasive Thoracic Surgery conference in Orlando, Florida.
Orlando, Florida
The conference started out with a grim statistic, reminding surgeons that only 45% of all lobectomies in the United States are performed with VATS (or minimally invasive techniques). With that sobering reminder, Dr. Scott Swanson, a thoracic surgeon from Brigham and Women’s in Boston, Massachusetts began the first session.
Dr. Shanda Blackmon from the Mayo Clinic in Rochester, Minnesota gave the first presentation, entitled, “Thoracoscopic Lobectomy in 2015: Can we teach it better?”
She used part of the presentation to discuss her recent STS paper on credentialing for minimally invasive surgery. She also spoke about how the recent developments in technology (3D printing, creation of better anatomic models, surgical simulators and telementoring) have changed the learning process.
Dr. Shanda Blackmon with Dr. Thomas D’Amico.
Unfortunately, this lecture was disappointing. While conceding that all of these techniques were inferior to a surgical fellowship, there was little discussion on how these techniques are affecting the learning process (or how well students actually learn using these techniques). It was more about the newest toys and less about the actual learning process. With the resident hours limitations, resident’s concerns about how this is limiting their exposures to a wider range of pathology as well as difficulty attracting surgical residents to the thoracic specialty, it would have been interesting to hear how effective these new technologies are at addressing these concerns. It would also have been interested to hear the downside of these technologies, or a debate regarding the recent STS paper. However, Dr. Blackmon more than acquitted herself with a later presentation on the management of bleeding complications.
“Technical Aspects in 2015: 16 years of progress”
Dr. Thomas D’Amico discussed the development and advancement of VATS over the last two decades. He reported that an increase in procedures being performed by dedicated thoracic surgeons as one of the reasons for improved outcomes. He also gave this as a reason for the increased number of VATS lobectomies since general thoracic surgeons are more likely to be experienced and comfortable performing this procedure (versus general or cardiac surgeons). He questioned the accuracy of data reported to the STS general thoracic database, which, as we’ve previously mentioned – is only utilized by a fraction of American thoracic surgeons. All of this information is a documented fact – and has been presented here at Thoracics.org before (with relevant citations).
However, he ventured into more tenuous territory when he questioned global statistics and stated that the United States is better than all of Europe in regards to the adoption and use of VATS technologies. While this is demonstratively true (as previously reported in Italy), it comes close to being dismissive and close-minded as to the contributions of the remainder of the world.
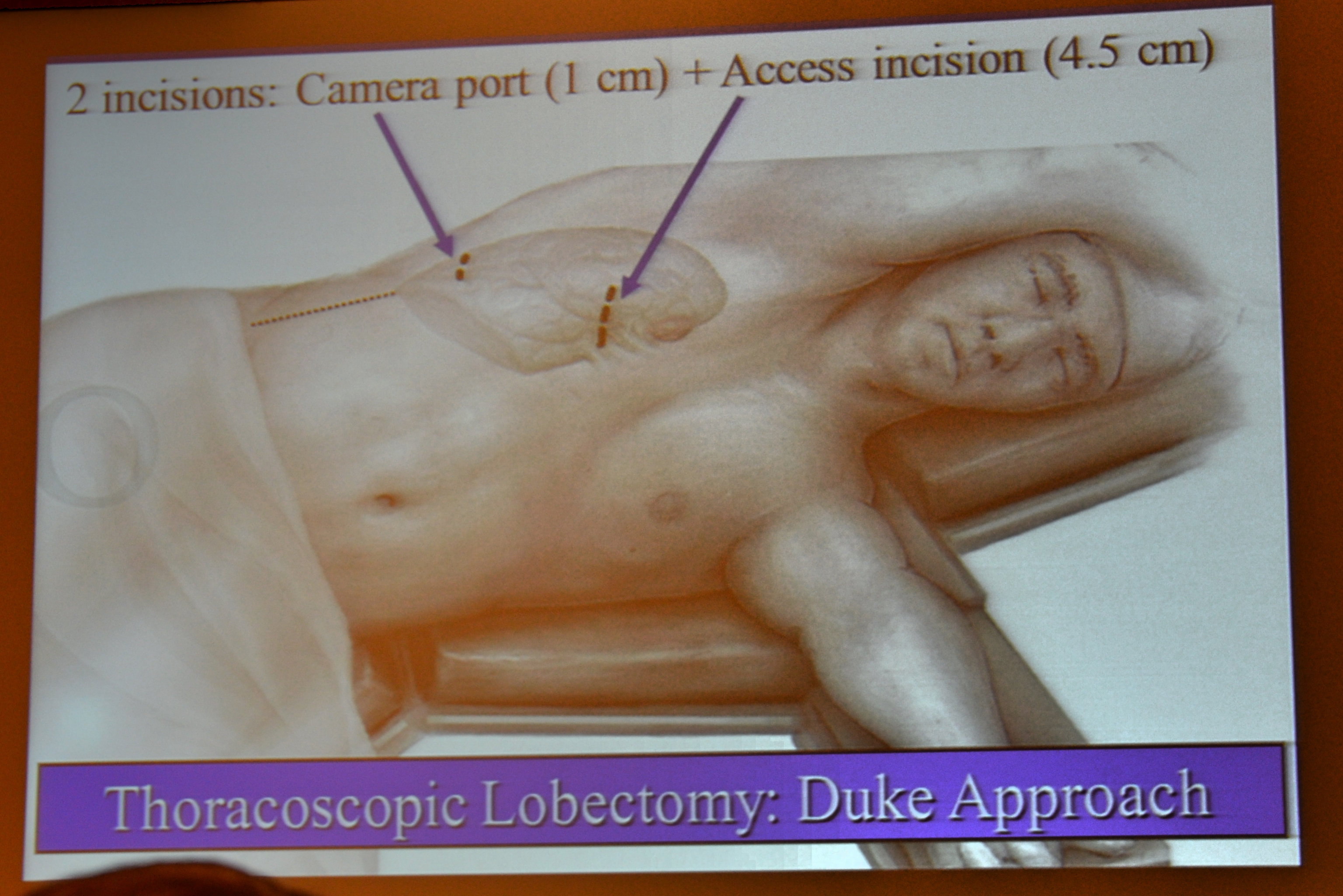
The Duke Modified Approach?
The most interesting point of his presentation was his announcement of the Duke appropriation of Dr. Diego Gonzalez Rivas’ Uniportal technique. In true American (and Duke) fashion, this was done in a backhanded style, as he announced the creation and adoption of a “Duke modified uniportal approach” which is actually a two-port approach (with the second incision being made in the same intercostal space as the initial incision).
Duke modified uniportal approach
He concluded his presentation with a review of the newest technologies in bronchoscopy, and biopsy procedures as well as a few hints for a successful VATS lobectomy.
He advocates for a full mediastinoscopy for lymph node dissection immediately prior to VATS, for both staging as well as ease of mobilizing the left main bronchus from this position, reminding surgeons that mediastinoscopy remains the gold standard for tissue diagnosis, despite being greatly underutilized in recent years.
He advises surgeons to routinely dissect the hilum and main pulmonary artery to increase their experience and comfort level in handling the pulmonary artery while performing VATS. Lastly, he states, “Do the easiest part of the operation first” and save the harder parts until the area has been cleared.
However, there were two standout presentations during the morning session.
The first was Dr. Diego Gonzalez Rivas’ presentation on non-intubated uniportal lobectomies. The second was Dr. Robert Cerfolio’s presentation on his experiences with Robotic thoracoscopic lobectomies*. As one of the most prolific thoracic surgeons performing robotic surgery, it was particularly illuminating.
Dr. Diego Gonzalez Rivaas, Dr. Scott Swanson, Dr. Thomas D’Amico, Dr. Robert Cerfolio, Dr. Shanda Blackmon, Dr. Todd Demmy and Dr. Mathew Hartwig. (photo provided by Dr. Blackmon)
The effect of Obamacare and the fiscal health of the American health care system and thoracic surgery
Reflecting many of the recent changes in the USA healthcare system, many of the presentations as well as the Question and Answer panels with the American surgeons were dominated by cost considerations.
Notably, Dr. Cerfolio used the term “save money” over 8 times to describe recent changes in techniques (using only bipolar energy versus staples to control the pulmonary vessels, for example) used while performing surgery with a two million dollar robotic system. But this “wal-marting’ of thoracic surgery is just part of general overall trend in American medicine and surgery which is forcing large-scale, and painful changes to American health care practices for financial and fiscal reasons under Obamacare, “pay-for-performance” measures and the new ICD-10 system. There will be more changes and adaptations as surgeons attempt to adopt these new federal mandates and institutional policies.