This fear of thoracotomies dwarfs the very real risks of prolonged illness and debility.
The story of empyema is as old as surgery itself. Hippocrates himself describes treating empyema with chest tube placement. However, over the years – the urge to treat this condition with the expediency and urgency it requires, has waned. With the advent of antibiotics came the idea of a “wait and see” philosophy. When the alternative was a thoracotomy, this could be forgiven. In the age of uniportal VATS, it is not.
Current treatment algorithm (with basic variations)
Patient w/ parapneumonic effusion/ empyema –> antibiotics –> still sick –> more antibiotics –> still sick –> chest tube (or pigtail placement) –> fibrinolytics then —-> If treatment fails, consult thoracic surgery
The current treatment algorithm, which often starts as several weeks of outpatient antibiotics, (usually initiated for treatment of community acquired pneumonia that develops into a parapneumonic effusion), that engenders an even longer period after subsequent follow up chest x-rays, then CT scan fail to show improvement.
A pneumonia in late September, becomes an effusion in October, then progresses to empyema as various strategies are attempted and fail. One antibiotic is switched to another, a pigtail is placed in radiology (with partial results), then perhaps, a larger tube, and fibrinolytics. Then, only then – is the thoracic surgery service consulted.
At this point, the patient has been sick for several days to weeks. As they remain sick, there is a decline in both nutritional and functional status. The “spry” and youthful 75-year-old becomes a mostly bedridden and frail elderly patient. This too, works against the patient and their recovery, as internal medicine physicians and pulmonologists are reluctant to refer this now frail patient due to the perceived rigors of surgery. This fear of thoracotomies dwarfs the very real risks of prolonged illness and debility.
For most modern-day practices, thoracotomies for decortication are a thing of the past. Minimally invasive surgeries such as VATS or uniportal VATS have replaced the large incisions of the 1980’s and reduced, if not eliminated, the incidence of morbidity and mortality related to this procedure. But our treatment algorithms haven’t kept up with surgical advances.
Proposed treatment algorithm:
Patient sick –> CT scan showing effusion –> thoracic surgery consultation with uniportal VATS for any effusion/empyema
Uniport VATS, (which is basically a glorified tube thoracostomy with anesthesia and a camera) allows for more than drainage of fluid from the pleural cavity. It also allows visualization, for better evacuation of infected material. Surgeons are able to target areas of loculation; and complete a full decortication, if necessary. While the use of anesthesia may add a degree of risk for the frailest of patients, it is the anesthetic/ and analgesic effects that allow for optimal patient positioning, and instrument manipulation, allowing for better results that bedside tube thoracostomy alone.
Why then, are we, the thoracic surgery service still only receiving consultations at the 23rd hour? Why isn’t the literature pushing for a change in perspective, or a change in practice?
Current literature on empyema
Chin, Redden, Hsu and Driel (2017, 2013) published a Cochrane review of multiple randomized control trials comparing outcomes for tube thoracostomy versus VATS. However, this review, which found in favor of VATS, was primarily based on pediatric studies.
Notably, this Cochrane review (which did not include uniportal VATS), showed decreased mortalityand length of stay in the thoracotomy and multi-port VATS groups compared with the tube thoracostomy group.
Another Cochrane study, Cootes et al. (2009), which also demonstrated a decreased length of stay, and decreased duration of chest tube placement with VATS) was withdrawn due to questions about inclusion criteria.
The remainder of the existing studies
The remainder of studies published since the Cochrane database review had similar limitations. A German study published in 2017 (Segerer et al.) that reviewed 645 children throughout the country that presented with empyema and showed no different in the length of stay. But only 7% of these children underwent surgical procedures compared to 46.9% that underwent lesser procedures (thoracentesis or chest tube placement).
A more recently published study, Tanbrawarsin et al. (2018) showed a decreased incidence in recurrent bacterial empyema in patients who underwent surgery, but it is difficult to apply these findings to our algorithm, since it was based on just 34 patients, and was not randomized. Furthermore, all advanced empyema patients received open thoracotomies. Some patients also underwent thoracoplasties, which is a procedure not commonly used in many parts of the world, including the North America.
Patients deserve better
While the published data appears to remain undecided on the algorithm, it is clear, our patients deserve better. They deserve an approach that is timely, and effective. There is significant data that demonstrates that early surgical intervention improves outcomes. But unless thoracic surgeons present an overwhelming mountain of evidence [at pulmonary and internal medicine conferences] that uniportal VATS is superior to lesser therapies, patients with empyemas will continue to receive lesser therapies, first, before we receive the thoracic surgery consult.
They deserve the opportunity to rapidly return to health and full function. For that, we need to commit to performing and reporting more research aimed at looking at the most effective treatment for empyema. We, in thoracic surgery, know that that the answer is not more of the same; increasingly ineffective antibiotic regimens and a long convalesce. Now, we have to prove it, and publish it, over and over, to get past the persistent belief that risk of surgery outweighs the risk of continued illness.
Now, we need to conduct and publish studies, and reviews that comparenonsurgical treatment with uniportal VATS (excluding the dread thoracotomy) and looking for meaningful end points beyond mortality. Studies need to look at the length of stay, chest tube duration, morbidities related to either treatment (deconditioning, blood transfusions, DVT, malnutrition, etc. ) as well as both the 30-day recurrence and re-admission rate.
Surgeons, this is your call to action.
References (with links to full text articles when possible)
Shresthra et. al. (2011). Evolving experience in the management of empyema thoracis. KUMJ 2011 Jan-Mar 9 (33) 5-7. In this study, 82% of patients treated with tube thoracostomy eventually needed thoracotomy. Full text link not available.
Tanbrawasin, A. et al. (2018). Factors associated with recurrent bacterial empyema thoracis. Asian J. Surg 2018 Jul, 41(4) 313-320.
There are multiple studies showing early surgical intervention improves outcomes in empyema, but only a single selection was placed within the editorial above.
Many of the modern masters of thoracic surgery were in Potsdam, Germany this June to discuss a myriad of topics in this year’s course until the heading of Troubleshooting. The lecturers included Dr. Diego Gonzalez Rivas, the inventor of the uniportal VATS technique, Dr. Alan Sihoe, a renown expert from Hong Kong, Dr. Timothy Yang from Shanghai Pulmonary Hospital, Dr. Marco Scarci, the creator of International VATS, and our host, Dr. Mahmoud Ismail. The course included both wet and dry labs so that surgeons unfamiliar with these techniques had an opportunity to apply what they learned during this and other sessions.
Standout presentations
Transcervical Uniportal VATS
Noted surgeon, and acknowledged expert in the area of transcervical VATS, Dr. Zielinski of Poland also gave a presentation on the transcervical uniportal approach, which is performed in the anterior cervical (neck) area. Using this collar incision, Dr. Zielinski is able to perform uniportal VATS for thymectomies and mediastinal operations as well as some lobectomies (generally upper lobes) and lung resections.
Dr. Zielinski talked about the challenges for this technique as well as the indications/ contraindications and potential complications while presenting data on his latest series of 32 patients. He gave surgical tips and tricks for using the transcervical approach, and how to avoid the most common complications.
There was a full session on setting up a uniportal VATS program with multiple speakers – along with troubleshooting the most common mistakes that surgeons (and their staff and administrators) make while starting a new uniportal VATS. They also talked about addressing the learning curve and ways to avoid common mistakes that occur during this period.
Common Complications after uVATS
Dr. Stefano Margaritora talked about how to prevent, detect and treat common complications after uniportal VATS. Drawing on his experience with over 1250 uniportal cases, Dr. Margaritora discussed the most common causes of bleeding such as dislodgement of vascular clips, bronchial artery bleeding, bleeding from lymph node harvesting sites and bleeding from the chest wall. He discussed the best ways to address this, such as use of newer anti-sliding clips, and the use of energy devices (like harmonic scalpels) for vessel sealing.
The ways to anticipate and prevent prolonged airleaks was also reviewed. Using anatomic fissures often lessens the incidence of airleaks post-operatively. The prevention of subcuatneous emphysema, as well as the relatively rare complication of lung hernia was addressed. Both of these complications can be reduced by meticulous and tight closure of the fascia at the conclusion of this procedure.
Using a serratus/ intercostal nerve block during this procedure is recommended to help reduce post-operative pain.
Dr. Firas Abu Ar spoke at several sessions – on both the use of uniportal VATS in pediatric patients as well as a case presentation on hydatid cysts. (Thoracics.org is planning to present this case study at a later date).
Hydatid cyst (photo provided by Dr. Firas Abu Akar)
There was a session on robotic VATs but with the exception of a discussion of preliminary trials of a robotic instrument that allows for uniportal VATS, most of the information has been presented on previous occasions.
The state of evidence for Uniportal VATS
Dr. Alan Sihoe gave an excellent presentation on the need more more randomized studies, and higher level evidence. “The time for case presentations on uniportal VATS is over.” As the leading academic researcher at this conference (as well as an active, practicing uniportal surgeon), and editor of multiple journals, Dr. Sihoe reminded attendees that as uniportal vats use continues to grow, and becomes a more common procedure, the types of articles surrounding the procedure need to advance as well. It’s no longer sufficient to submit papers like case reports where the purpose of the paper is to explain the procedure, and basically say, “look at this cool case I did.” Surgeons need to move beyond these sophomoric writings to produce high quality, high value papers that add to the body of scientific literature around uniportal VATS. He then gave the audience specific, helpful guidelines and advice on designing, writing and submitting articles for publication.
Attending watching the first of two live cases
After the didactic portion was completed, there were two live cases streamed from the local hospital for surgeons to review along with the dry and wet labs.
a Mexican surgeon using one of the newest tumor located/ marking systems during one of the dry labs
Note to readers: This will be the last article on uniportal VATS training. This topic has been extensively covered thru this and other posts here at thoracics.org. For more information on the essentials of uniportal VATS training, please review our archives under meetings and conference coverage.
Additional references
Eckland K, Gonzalez-Rivas D. (2016). Teaching uniportal VATS in Coruña.J Vis Surg. 2016 Mar 11;2:42. doi: 10.21037/jovs.2016.02.25. eCollection 2016. PMID:29078470
Today’s recommended read is for all of the thoracic surgeons out there that are interested in establishing their own nonintubated uniportal programs. This is a interesting article if you’ve taken a masterclass on uniportal technique, reviewed the literature around nonintubated surgery, but haven’t yet taken the next step to start performing this procedure at your hospital.
Thoracics.org has reached out to the corresponding author, Sook Sung for more information about their experiences with nonintubated uniportal VATS including some updates, but let’s review the primary article while we await a reply.
In the article, Nonintubated uniportal video-assisted thoracoscopic surgery: a single center experience, Seha Ahn et al. discuss their experiences over a six month period after initiating this technique in January 2017.
During this period, 40 patients underwent this technique. Pre-operative patient selection was important with multiple exclusionary criteria.
Exclusionary criteria for initial cases: General
Obesity (BMI greater than 30
Anticipated/ expected difficult airway
Persistant cough/ or high amount of secretions
At increased risk of gastric reflux
Exclusionary criteria: Cardiopulmonary
Expected/ anticipated to have extensive adhesions
Prior pulmonary resection
N2 stage lung cancer
Severe cardiac dysfunction (exact definition not defined)
Photo by 서울성모병원
Anesthesia and Intra-operative Monitoring
Prior to the procedure, patients received dexmedtomidine. At the time of the procedure, patients were maintained with infusions of remifentanyl and propofol.
No patients were intubated. Patients did receive supplemental oxygen by mask at a rate of 6 to 9 liters/ min. Oxygenation was monitored with botha small single nostril end-tidal CO2 monitor and pulse oxymetry. Anesthesia monitoring including a BIS monitor. General hemodynamic monitoring consisted of continuous EKG/ telemetry and serial blood pressure cuff measurements.
Surgical technique
As part of the surgical technique, the authors administered an intercostal nerve block for additional analgesia. In the majority of patients (35 of 40), intrathoracic vagal nerve blocks were also performed to reduce / prevent coughing during the procedure.
The procedure was carried out using a single 3 to 4 cm incision. The main surgical instruments used were a 10mm 30 degree scope, a harmonic scalpel and a curved suction tip catheter.
Results
General demographics
There were 40 total patients in this study, which spanned a period of six months. More than half of these patients (57.5%) were women. The mean age was 60.
The vast majority of these patients (72.5%) had lung cancer. Seven patients (17.5%) had surgery for pulmonary metastasis. The remainder of patients had surgery for either benign lung disease or pleural disease.
Procedure types
Over half of the patients underwent lobectomies (57.5%). 10 patients (25%) had wedge resections, with six patients having segmentectomies (15%) and a solo patient undergoing a pleural biopsy.
Complications
There were several intra-operative conversions. The majority of these conversions were related to anesthesia, with 3 patients requiring conversion to standard intubation. The authors are a little unclear with the reasons for this – with one sentence saying it was not related to hypoxia (with all patient sats greater than 90%). The authors then attribute the conversions to excessive respiratory movements, but then report that all three of the patients’ hypoxemia resolved with intubation. This is better explained in a later portion of the paper, but it is still a bit confusing as to whether excessive respiratory movement was a contributing cause for the reason to intubate mid-procedure.
There was only one conversion for surgical technique, which occurred after the dread pulmonary artery injury, with the authors converting to multi-port VATS. There were no conversions to open thoracotomy.
Post-operative complications
Seven total post-operative complications (17.5%)
3 patients with prolonged air leaks
2 chylothorax
1 delayed pleural effusion
1 pneumonia
Interestingly enough, outcomes based on traditional criteria, (chest tube days, and overall length of stay) were not significantly different that results published for more traditional types of thoracic procedures.
The average post-operative chest tube time was 3.2 days (range: 1-13 days)
The average hospital stay was 4.4 days (range 1 – 18 days).
There was one notable outlier listed, a patient with a prolonged airleak that resulted in a 20 day hospital stay.
Discussion
This article is note worthy of several reasons, in that the authors both describe their techniques and the initial results of the initiation of a new surgical approach (nonintubated and uniportal) in their facility. The authors are to be commended for reporting research results that show a (17.5 %) high rate of complications, which is presumably related to the learning curve of adopting a new surgical protocol.
However, this article would have been much more informative if there had been more of an in-depth discussion of the challenges involved in initiating and managing a nonintubated uniportal program, instead of a general review of the literature. While the article notes that there was a solo surgeon involved in these 40 procedures, there is little discussion of the prior experience of that surgeon or the anesthesia team(s) involved. What the surgeon previously experienced in uniportal VATS? If so, what was the level of experience?
The same goes for the anesthesiologists involved in this study, since a large portion of the procedure (ie. the nonintubated portion) as well as the highest level of conversions (to standard intubation) occurred under their guidance. A short discussion about intra-operative intubation would have been a helpful addition for readers as well, such as a discussion of the difficulties (or lack thereof) of intubating a patient after they have been secured into a lateral decubitus position.
While the traditional outcomes measures appear fairly unchanged in comparison to standard VATS with general anesthesia and intubation, what was the difference in related outcomes?
Was there a difference in/ would they anticipate a difference in (with larger numbers of patients):
Post-operative intubation? How man patients required urgent/ emergent intubation during the post-operative period?
Post-operative pneumonias and other respiratory complications? While the authors cite one post-operative pneumonia, there appear to be few other respiratory complications cited in this study.
Post-operative anesthetic complications such as hemodynamic compromise (requiring prolonged use of pressors, for example). What about post-operative nausea/ vomiting or gastric ileus?
Since nonintubated and uniportal techniques have been proposed as a alterative to standard surgery for high risk patients (patients with poor respiratory reserve/ cardiovascular disease), the presence or lack of these complications in patients (even specially selected patients) is important.
When reviewing the lack of clear-cut advantages such as shorter length of stay, were there other reasons for it, such as post-operative nursing care? Are there changes that need to be implemented/ have been implemented since this study was published that have resulted in fewer chest tube days, or a shorter overall length of stay?
In the time since this study was concluded, what have been this group’s continued experience? Have there been any unexpected outcomes or observations? What changes continue to need to be addressed?
Are there any other observations that the authors would like to share? While traditional journals have size and article length limitations, we don’t here at thoracics.org.
Ospedale San Gerardo, site of International VATS 2018 is located in Monza, just an hour outside of Milan
Monza, Italy
Dr. Scarci has returned to his native Italy, and his first-born child, the International VATS Symposium has come with him. Now the chief of thoracic surgery at the 1,000 bed Ospedale San Gerardo, Dr. Scarci has again managed to assemble many of the world’s best and brightest in thoracic surgery.
Over 130 attendees participated in the live surgery, and lab event – with a multitude of other participants watching and commenting thru the CTSnet.org Live Streaming feature. While the majority of on-site attendees were from Italy, there were attendees and lecturers from around the world, including Myanmar, Panama and Pakistan.
The overarching theme of this year’s conference was segmentectomies (sublobar resections) but there were standout presentations in all areas.
The segmentectomy series of lectures discussed the differences between a wedge resection and a more anatomical sublobar segmentectomy). Piergiorgio Solli was not pleased to give his lecture on the anatomy and nomenclature of segmentectomies, and it showed. The usually composed surgeon was visibly irritated during his presentation.
Dr. Gaetano Rocco
The modern-day inventor of uniportal thoracic surgery, Dr. Gaetano Rocco discussed the latest data on morbidity and survival with segmentectomy. Formerly of Naples, but now representing Sloan Kettering in New York, made a point to discuss the difference between intentional segmentectomies (suitable for ground glass opacities and very small limited cancers) and “compromise” or forced segmentectomies, which are lung resections performed on patients with very marginal lung function. These forced segmentectomies are concerning for adequate margins.
He reminded surgeons that the scientific data isn’t always supported by our practice – while segmentectomies are superior to wedge resection, surgeons are doing wedge resections much more often even though the decrease in lung function (FEV1) after segmentectomy is only transient and limited in nature. He also reminded surgeons that no matter the operation, adequate lymph node sampling was essential and that to some extent survival is based not just on adequate staging (via proper node sampling), and good margins, but on the physical location of the primary tumor, (with subcarinal and basilar based tumors carrying the best survival.)
Alex Brunelli and Dr. Marco Scarci debated sublobar resection versus lobectomy on several different points – with Dr. Brunelli reminding the audience that segmentectomies are just 5% of all lung resections, and that 75% of all procedures performed in Europe continue to be open procedures – so that theoretical discussions on research findings as well as minimally invasive techniques (in general) aren’t being replicated in real world practice for the majority of surgeons.
Dr. Piergiorgio Solli discusses the anatomy and naming of pulmonary segments for resection
Sublobar resections in the “Compromise” patient
Dr. Scarci discussed the current literature and evidence regarding respiratory outcomes on patients undergoing sublobar resections versus lobectomy. Surprisingly, in the majority of these studies, the difference in post-operative lung function is very small – and transitory. He discussed several of the limitations in currently published research which may have skewed some of these results, but that [at present] there is a lack of clear evidence to support the use of sublobar resection for preservation of pulmonary function.
Nodes, nodes and more nodes
Luca Bertolaccini gave an interesting lecture on lymphadenectomy in segmentectomies – which boiled down to: take more nodes. Do a complete and thorough lymph node dissection – and take at least TEN nodes.
Dr. Dunning: Fantastic style but still leaves you hungry
As usual, Dr. Dunning’s dramatic and charismatic style meant that he could argue just about anything in thoracic surgery and successfully acquit himself. But not without hurtling a live grenade into the audience – criticizing Gonzalez Rivas and his adherents multiple times for slavish devotion to uniportal techniques.
I guess without Dr. Lim there to make thoughtful and logical arguments during the conference, someone had to stir up a ruckus. Who better than thoracic surgery’s own Pied Piper? Part showman, and part infomercial salesman, Dr. Dunning did his best to argue for open surgery using the “It’s not the size of your incision, but the quality of the post-operative care” argument.
Despite his whimsical delivery style, Dr. Dunning was able to deliver the data – reams of it. Unable to resist a dig at the absent but larger-than-life Robert Cerfolio, Dr. Dunning repeated last year’s technique and cited a mountain of Cerfolio’s work in his defense of the humble thoracotomy, all while assuring the audience that “it’s not your grandfather’s thoracotomy.”
Using that thread, he went on to remind attendees of the importance of ongoing work in the area of massive resections for advanced cancers. He presented a myriad of published titles highlighting major chest wall resections and advanced techniques for metastatic disease.
His always enjoyable delivery style as also punctuated with praise for another one of the speakers, Dr. Joao Carlos Das Neves Pereira, and his “extreme rehabilitation” program. He also made a point of highlighting the published works of surgeons outside of the traditional confines of Europe and the United State, focusing on contributions of our colleagues in Brazil and Asia.
While it was a great lecture, it left the audience feeling a little bit hungry for more substance, instead of a remote control like flashing thru channels. It was the perfect set up for the end of the day lecture by Dr. Das Neves Periera. Too bad there were something like 12 other presentations between the two.
The fourth VATS International Symposium is this October 20th – 21st, 2017. As readers know, this course has been highly recommended in the past by Thoracics.org.
The preliminary program has been released, and it looks like audience favorite and straight shooter, Eric Lim will be opening the conference.
Italian thoracic surgeon, and the inventor of the first uniportal VATS procedure, Dr. Gaetano Rocco, along with the prominent American surgeon, Dr. Robert Cerfolio will also be presenting. There will be several presentations comparing uniportal VATS with robotic assisted surgical techniques (RATS). But this is more than an academic discussion – in addition to notable speakers, the conference includes live cases, practical tips and hands-on training.
Representatives from Storz will be speaking to thoracic surgeons on caring, repairing and maintaining thoracoscopic equipment. There are still spaces available for attendees, including the state-of-the-art wet lab. This wet lab offers surgeons the opportunity to try new techniques using 3-D models, while proctored by leaders in the field.
The first ever Thoracics.org Award to recognize innovation and achievement in thoracic surgery is now accepting submissions.
The Thoracics.org VATS International Award
Thoracics.org is pleased to announce our first international award for innovation and achievement in thoracic surgery. This award is designed to recognize and encourage research and publication in the area of VATS, including uniportal VATS.
This award is being offered by thoracics.org for a previously unpublished paper, study or case report on any aspect of thoracic surgery involving VATS (video-assisted thoracoscopic surgery). Topics can include case reports on complex cases, use of VATS in specific populations or disease conditions, unpublished research results / retrospective analyses or similar themes.
This award will be presented at the VATS International conference in London, UK on October 20 – 21, 2017.
Award Sponsors
This year we are honored to be sponsored by VATS International and Dr. Marco Scarci.
VATS International 2017 – We’ve written about this conference in the past, so thoracics.org is very excited to be able to present the Thoracics.org award at the 2017 conference. This year’s roster of speakers and topics includes some of our favorites, as well as introducing some timely new topics such as certification in minimally invasive thoracic surgery.
The Thoracics.org award to be presented at VATS International 2017
Dr. Marco Scarci – Dr. Scarci is a thoracic surgeon at the University Hospital of London and the founder of VATS International.
Rules:
Deadline: All submissions must be received by June 1, 2017 at 8 am eastern standard time.
Authorship: Papers must be the work of a sole author, and each author may only submit one entry. Entries are limited to practicing specialty thoracic surgeons, and surgeons completing their thoracic surgery fellowships. This contest is not open to general practice surgeons, or non-thoracic surgery specialties.
Originality: All entries must consist of previously unpublished work. Evidence of prior publication of material submitted for consideration is grounds for immediate disqualification.
Entry format: Entries consist of three (3) parts; the paper, the title page and the CV. Incomplete or partial entries may be ineligible for the award.
A. Paper specifications:
Papers must be written in English.
Maximum length is ten pages double-spaced with a 12 point font.
All submissions should be in Microsoft Word or a similar PC compatible type document. No pdfs will be accepted. Multi-media materials such as photographs, or short video clips may be attached to the paper for inclusion in the on-line publishing format. Video clips should be less than 10 minutes in length. No individually identifying information should be included in submitted photographs or videos.
B. A separate title page should be included with the essay.
This title page should contain:
-Author’s name
-Contact information including physical address, email and telephone number
-Institutional or Academic affiliation(s)
-Name and contact information of immediate supervisor
C. (Optional) – Author photograph – as a separate attachment, labeled as first initial_lastname.
D. A current curriculum vitae (CV) should also be submitted as part the entry package, as a separate attachment.
Send all submissions to: k.eckland@gmail.com
Publication:
All entries are submitted for publication at thoracics.org as a guest post. These posts will be published with the author of each paper to remain anonymous until the award winner has been announced. The winner of the Thoracics.org Award will be posted on thoracics.org on August 1st, 2017.
Following the announcement of the name of the recipient of the Thoracics.org Award, on-line articles will be amended to include author information, including name, affiliation, location and author photograph (if included with the original submission).
Judging:
Judging of the entries received will be done by a panel of thoracic surgeons. The names of the members of the panel will be revealed at the awards ceremony. While visitors to thoracics.org may comment on published entries, these comments will not be part of the judging criteria.
The Award:
Thoracics.org award
The award will be presented in person at the 2017 VATS International conference in London, England.
In addition to receiving recognition within the international thoracic surgery community, the award recipient will receive*:
Complimentary registration to the 4th annual VATS International conference in London, UK. This course is one of the best courses on uniportal and minimally invasive thoracic surgery and includes content on uniportal vats, robotic surgery, awake and nonintubated surgery, and other minimally invasive techniques. The lectures are given by the masters of these techniques, including the master of uniportal surgery, Dr. Diego Gonzalez. This year’s preliminary line up of speakers and topics looks like another stimulating session of minimally invasive techniques interspersed with timely discussions on current issues in VATS (Registration courtesy of VATS International).
A copy of the new textbook, Core topics in thoracic surgery.
Core topics in thoracic surgery
Core Topics in Thoracic Surgery provides accessible and concise coverage of the topics most often encountered in thoracic surgery practice. This handbook will guide the reader through revision of the topics covered in the FRCS(CTh) examination, and also covers more specialist topics in detail. In-depth technical sections offer guidance for difficult procedures, with useful commentaries from leading surgeons. A broad range of thoracic surgery issues are examined, with the latest evidence and information relevant to the speciality presented in a clear fashion. Combining an easy-to-use revision guide for trainees and a comprehensive reference text for cardiothoracic surgeons and recently appointed consultants, this is a one-stop guide to thoracic surgery. Authored by leading experts in the field, this resource will be invaluable to cardiothoracic surgeons, respiratory physicians and specialist nurses seeking to refresh or expand their knowledge of this field. (Textbook courtesy of Dr. Marco Scarci).
Additional sponsors include:
*Corporate and individuals wishing to co-sponsor this award may contact k.eckland@gmail.com
If you can only attend one thoracic surgery conference, shortlist VATS International.
Attendees with Dr. Marco Scarci (2nd from the left)
VATS International
VATS International (previously known as Cambridge VATS) is the brainchild of Mr. (Dr.) Marco Scarci. The Italian surgeon recently made the switch from NHS Papsworth (Cambridge) to the historic Royal London Hospital. Each year, Dr. Scarci gathers the world’s specialists on minimally invasive surgery to meet here in the United Kingdom to share knowledge and practice techniques for traditional VATS, uniportal approaches (standard and subxyphoid) and robotic surgery.
This is the third year of the conference and it’s reputation for dynamic speakers and controversy continues. With over 100 attendees, and a wide range of global participation as well as live surgery sessions and a wet lab, Dr. Scarci has had runaway success despite some last-minute challenges posed by his recent defection from the Cambridge facility. (Having met several members of the rather staid and traditional thoracic surgery department at Cambridge, Dr. Scarci, with his emphasis on minimally invasive surgery, is undoubtedly better-suited to the London-based facility).
Excellent lecture content, dynamic speakers
There were several excellent speakers, making it difficult to narrow the selections for presentation here. The obvious standout was Dr. Lim, (as discussed in a previous post).
As one of the course directors, and the inventor of the uniportal approach, Dr. Diego Gonzalez Rivas gave several lectures on the technique aspects of uniportal VATS.
Dr. David Waller followed up with a lecture entitled “Intra-operative problems in VATS lobectomy: Avoidance and Management.” He discussed complicating patient factors such extensive adhesions, anthrocotic lymph nodes, anatomical variance and incomplete fissures that increase the complexity of uniportal cases. He also identified common surgical problems such as difficulty identifying the target lesion, development of large air leaks and inadvertent damage to hilum or bronchus with strategies to prevent & manage these issues. He reviewed surgical techniques on bleeding control/ major vascular injury as well as absolute indications for surgical conversion such as equipment failures, airway injuries and stapler jams. In closure, he also warned against using conversion rate as an outcome measure. It was a fairly dry lecture despite being an interesting and important topic.
Among the remaining speakers, the overwhelming theme of change, and evolution along with an underlying sense of defiance continued. These surgeons are here to discuss, learn and practice uniportal surgery even if more traditional surgeons don’t approve.
Some of the best presentations were:
Dr. Alan Sihoe, (Hong Kong) gave a modified lecture called “Reasons not to perform uniportal VATS lobectomy”. This lecture which was adapted from a previous lecture from last year’s conference also addressed criticism of uniportal VATS. He reviewed the existing literature on uniportal surgery which suggests that uniportal surgery is a safe alternative to other surgical approaches.
Dr. Alan Sihoe
During the lecture, Dr. Sihoe encouraged surgeons to move past case reports to performing higher level research such as randomized control studies to create evidence in the area of uniportal surgery. He also encouraged participation in the European database, to gather prospective data on uniportal surgery. Until there is a larger body of literature utilizing higher levels of evidence, uniportal surgery will continue to face significant (and justifiable) criticism as a fad procedure. While it wasn’t a ground-breaking lecture by any means, it was also a reminder for thoracic surgeons to think like a researcher. It was a good follow-up on Dr. Lim’s opening lecture.
Dr. Gaetano Rocco (Italy).
Dr. Rocco, one of the pioneers of the uniportal approach, continued the discussion of the need for evolution and adaptation but with a different approach in a talk entitled, “VATS major pulmonary resection for (very) senior surgeons. He extended an olive branch to older, experienced thoracic surgeons with limited experience with VATS. His lecture discussed the ways to remediate older surgeons, and build their skills and comfort level in performing VATS procedures. His lecture offered a clear-cut and concrete , step-wise curriculum and self-assessment tool for surgeons looking to improve their VATS skills, starting with VATS lobectomy.
Dr. Gaetano Rocco (left)
Dr. Ali Khan (India) delivered two lectures, the first on operating room technology, but it was the second on uniportal surgery for inflammatory and infectious diseases that really piqued my interest. Part of this is due to my interest in the surgical treatment of tuberculosis, and my great appreciation for empyema as a surgical disease. Most readers know that reducing the time from presentation/ diagnosis of empyema to surgical decortication is one of my goals in daily practice, so any reminder that the morbidity/ mortality of decortications have been greatly reduced by minimally invasive surgery is always welcome.
Dr. Ali Khan
Honorable mention: Dr. Alex Brunelli, “Fast track enhanced recovery for MITS”. Basically a talk on care plans with specific markers for timely progression and discharge. While this is standard fare for nurses, the use of care plans for many surgeons is unfamiliar territory. It would have been nice if the care plans were available as a handout for surgeons who are still fine-tuning their own programs. It also would have been nice for a better breakdown of how specific items reduced the length of stay (how/ how much) or decreased the rate of complications. Nice to mention care plans but better to have measurable and specific examples.
After the extensive lecture series on the first day of the conference, the second day was devoted to live surgery cases and the practice lab.
Wet Lab
Since animal research of any kind is tightly controlled in the United Kingdom, 3D printed models were used for the wet lab portion of the course.
3D model of thoracic cavity
This is the first time that this type of model has been used. While the green plastic housing looks rudimentary, on closer inspection of the ’tissue’ inside, one gets a better appreciation for the models. The tissue is soft, and sponge-like. The lung doesn’t inflate but appears more lifelike than other models.
I don’t have the patience or temperament to shoot video footage, but I did record a couple of seconds so readers could have an idea what the wet lab portion of the course is like. In the video, Dr. Sihoe is instructing two trainees on the proper technique.
Despite its relative youth, VATS International remains one of the best conferences on minimally invasive surgery, inferior to none. This conference is highly recommended and considered superior to many of the traditional conferences on the topic (such as the annual Duke conference), due to lecture content on timely topics and controversial issues. The hands-on wet lab and participation by internationally recognized and globally diverse speakers makes this conference more valuable to attendees looking for exposure to newer surgical techniques.
Thoracics.org 2017 wish list
What would I like to see next year? As mentioned above, VATS International is one of the better courses available for surgeons interested in uniportal, subxyphoid and other minimally invasive techniques. But there is still more content I’d like to see – on nonintubated and awake surgery, for example.
However, with regards for this year’s speaker, an anesthesiologist from Papsworth Hospital, this topic would be better covered by one of the “masters” of the field; Dr. Eugene Pompeo of the Awake Surgical Group or Drs. Hung & Chen. The “Papsworth Experience” per se is limited to heavy sedation/ general anesthesia without mechanical ventilation. Patients still have LMAs and are heavily sedated. One of the main benefits of nonintubated anesthesia is the ability to operate on the medically fragile. It would be enlightening to hear more about operating on this population from more experienced clinicians. One of the topics that has been essentially ignored in the literature on this topic, is the implications for thoracic surgeons, anesthesiologists, operating room and recovery room staff on operating on this population of sicker patients. I think readers would like to hear about the new challenges in managing patients that were previously inoperable due to serious co-morbidities.
A discussion on developing or actualizing a formal certification process with examination for minimally invasive surgery with suggested curriculum, and case log requirements would be a nice addition. Blackmon et al. published a credentialing guideline but it’s a multi-part overly complex document full of “levels” of competency. I’d like to see a discussion on the development of an actual certification to be offered by a surgical licensing body or surgical society. Since the American agencies would probably take another 20 years to consider the idea, perhaps one of the guest speakers’ native society would be more willing to take on this project?
I’d also like to see at least a limited amount of content on esophageal surgery. I know, I know..While practice areas for thoracic surgeons vary around the globe, with the rapid rise in esophageal cancer, a lecture on the role of minimally invasive surgical techniques for esophageal surgery would be a great addition to the current roster of topics, particularly if it was given by one of the modern masters of esophageal surgery like Dr. Benny Weksler or Dr. Roy Chen.
Lastly, one of the most enjoyable aspects of this conference is the truly international flavor. Watching a surgeon from Israel demonstrate uniportal techniques from a practice site in Shanghai brings home the importance of global collaboration. Hearing surgeons from India, Brazil, France and Canada present data on their practices is critical to gain perspective, and exchange ideas. It also helps prevent attendees from falling into the trap of “we’ve always done it this way.” This concept could be expanded to include designated global snapshots, to highlight research or data in specific geographic areas, like Dr. Khan’s lecture on uniportal approaches for infectious and inflammatory disease.
A full lecture on cost containment techniques for surgeons practicing in hardship areas would be a great topic. Dr. Sihoe touched on the issue during one of his lectures, but since I’ve heard other surgeons talk about the limitations posed by having only one thoracoscope, I’d love to see an equipment representative give a lecture on maintaining thoracoscopes, where to donate old scopes or how to rehab these scopes for a second life. A talk about modifying existing surgical instruments for surgeons who can’t afford the Scanlan set would be helpful as well. One of the reasons these courses have been so successful it the fact that they are technically based, so adding a section like this might help spread the uniportal technique to a whole socio-economic and geographic segment of patients that it might not otherwise reach.
This last item might be a tall order for Dr. Scarci and his group but he’s done pretty well thus far.
There were plenty of reasons for surgeons from all over Latin America to converge on Cuscu, Peru for the 2nd annual VATS PERU Uniportal Master Class, which covered the basics of the uniportal approach as well as nonintubated and awake uniportal surgery. There were subxiphoid and uniportal cases streamed live from Shanghai Pulmonary Hospital. But beyond the usual reasons of networking, discussing and sharing case knowledge, and the presentation of research findings and evidenced-based practice, there were several reasons why VATS Peru was more than just your average regional thoracic surgery conference.
Why attend VATS Peru? The three best reasons:
1. The wet lab – which allowed surgeons and their surgical assistants to apply the theoretical knowledge they learned during the first two days of lecture in operating room scenario en vivo. The “en vivo” is critical, fancy simulators aside, there is no better challenge to ‘book knowledge’, and application of practical skills than in the scenario of an operating room, with real models and active bleeding.
A surgeon in the master course receives instruction from Dr. Diego Gonzalez Rivas
2. Lectures from the master surgeon himself; Dr. Diego Gonzalez Rivas: That’s where the second critical component comes in, in the form of the candid, direct and straight-forward lecture by Dr. Diego Gonzalez Rivas on Control of Inter-operative Bleeding. If you weren’t paying attention during this lecture, it’s obvious in the lab. This isn’t a computer course where you can dial in your answers, fast-forward thru lectures and print off a shiny new certificate. This isn’t a computer app, or a simulation that you can reset and re-start as soon as the surgery heads off course, to try again.. It’s real surgery.
3. Dr. Carlos Fernandez Crisosto
Lastly, if you didn’t attend VATS Peru, then you missed an opportunity to know and to talk to Dr. Carlos Fernandez Crisosto. VATS Peru is his brainchild, and the organization was created specifically to advance minimally invasive surgery in Peru. VATS Peru is separate from ALAT (the Latin American Society of Thoracic Surgeons), of which Dr. Fernandez is the current president. VATS Peru is also separate from the Peruvian Society of Thoracic Surgeons which has its own focus in the thoracic surgery specialty.
Dr. Carlos Fernandez Crisost0, Cardiothoracic and Vascular surgeon
Dr. Fernandez, a Tacna native, works at Daniel Alcides Carrion Essalud facility in the southernmost region of Peru. He is the sole cardiovascular and thoracic surgeon for the city of Tacna, and performs cardiac, vascular, and endovascular surgeries in addition to general thoracic surgery. While he is a trained cardiovascular surgeon, (in addition to general thoracic) thoracic surgery is what he enjoys most.
He trained in Argentina, and practiced in Cordoba, Argentina for 23 years before returning to Tacna in the last few years.
His average case volume is around 380 surgeries a year, and he reports that all of his thoracic surgeries are generally performed using the uniportal thoracoscopic approach. He also does transplant, which requires him to travel to Lima specifically to perform the procedure. The transplant program is small and performs 4 to 5 transplants per year.
In his practice he sees the usual oncology cases, and empyemas but he also sees a large number of patients with tuberculosis, as well as an assortment of hydatid cysts, and pectus cases. Trauma from accidents, as well as injuries from guns, and knives also comprises a large part of his practice.
Dr. Fernandez is pleased with the success of his course, since this is only the second time the course has been available here in Peru. It was a complex logistical arrangement to hold the course in Cusco this year, but with the help of his wife, a professional events planner, they were able to pull of the event with very few hiccups. Next year, they plan to hold the event in Lima, the capitol of Peru and a city famed for its gastronomic offerings.
If you missed this year’s VATS Peru, look for VATS Peru 2017 here at Thoracics.org next fall.
Day One of the VATS Peru 2016 Conference was a primer for surgeons interested in learned and performing uniportal VATS. Dr. Gonzalez Rivas’ lectures formed the basis of theory and principles of uniportal thoracoscopic surgery, with additional lectures by Dr. William Guido, Dr. Timothy Young and Dr. Deping Zhao.
Surprisingly, many of the surgeons at the event informed me that they already use some uniportal techniques in their practice. But they came here to Cusco, Peru to learn more from the Master of Uniportal surgery himself, Dr. Diego Gonzalez Rivas before attempting more complicated and complex surgical cases like sleeve resections. Others came to learn more about nonintubated surgery in their uniportal patients. The remainders were the core group of surgeons who came to get their first taste of uniportal surgery.
Some came from the local areas; from Lima, from Chile, and Ecuador. Others came from other parts of Latin America; from Mexico and Costa Rico. There was even a practicing surgeon from the United States, who realized that if he wanted to pursue the most advanced surgical techniques and minimally invasive surgery in thoracic surgery, that he couldn’t do it at home. That’s a big paradigm shift for a surgeon from a nation that tends to think if it wasn’t invented in the United States, that it doesn’t exist, or has no merit. It is also, from my perspective, a welcome change.
With Dr. Tim Young, Dr. Diego Gonzalez Rivas and Dr. William Guido
In the five years that I have been travelling the globe, writing about surgical innovation, I am usually alone in my quest, in seeking innovation outside of American medicine. That’s not to say we(Americans) don’t have our own great surgeons – I can easily rattle off quite a few – but it’s an acknowledgment that surgical innovation (or any innovation in general) is not the exclusive domain of the United States. That sounds like a fairly basic principle, but one that is rarely seen in practice. American doctors and nurses just don’t attend international events to learn. They only attend to teach – and often leave as soon as their lecture is complete, ensuring that an accidental opportunity to be exposed to new ideas is minimized.
So it was a pleasure to meet the surgeon from California, who took time off from a perfectly successful practice performing routine thoracotomies, to learn more about uniportal surgery at this and another upcoming master course.
VATS Peru 2016 – learn uniportal and subxiphoid techniques in the wet lab, at the hands of the inventors of these techniques at this year’s conference in Cusco, Peru.
Cusco, Peru – September 2016
The 2016 VATS Peru conference and wet lab is scheduled for September 7th – 9th and this year’s agenda looks to be interesting and exciting.
Dr. Carlos Fernandez Cristoso is this year’s director of the course, and he has all the essentials of uniportal (single port thoracic surgery) VATS including special sections on : Management of intraoperative bleeding, difficult / advanced uniportal cases, and uniportal VATS on awake and nonintubated patients in addition to much of the standard uniportal fare.
Dr. Diego Gonzalez Rivas is honorary president of the course.
The course also includes lectures on the uniportal subxiphoid approach, as well as how to teach uniportal approaches to residents and fellows. The surgeons of Shanghai Pulmonary Hospital as well as Dr. Diego Gonzalez Rivas , the inventors of subxiphoid and uniportal approaches (respectively) will be there. The surgeons of Shanghai Pulmonary Hospital will be sharing their experiences of performing over 8000 uniportal resections a year, as well as presenting a live case direct from Shanghai during the conference.
Also – this conference is unique in offering an opportunity for surgical assistants, and scrub nurses to gain insight and share experiences in uniportal techniques with concurrent courses scheduled for operating room nurses. Both sections spend the last day of the conference in the wet lab applying newly learned techniques.
To register for this course – click here or e-mail : consultas@vatsperu.org
Learn Uniportal VATS from the masters – with a hands-on wet lab..
Attendees at the November 2015 course
La Coruna. Espana
Beyond the theoretical
The Advanced course on uniportal VATS differs from the rest of the courses covered here at Thoracics.org in that it goes beyond didactic lectures and surgical demonstrations. The three day course, sponsored by Johnson & Johnson is one of the few to offer hands-on training in a one-day ‘wet lab’.
Dr. Dario Amore (Hospital Monaldi, Naples, Italy) operates under the watchful eye of Dr. Maria Delgado of Hospital Universitario de Coruna.
During the lab portion of this course, attendees are encouraged to perform several lobectomies using the uniportal approach while being proctored by several well-experienced surgeons including Dr. Diego Gonzalez Rivas himself, and his surgical colleagues (Dr. Maria Delgado Roel, Dr. Mercedes Del la Torre and Dr. Ricardo Fernando Prado). These surgeons make up the world famous thoracic surgery department at the Coruna University Hospital. They are joined by Dr. Miguel Congregado, another Spanish surgeon from Seville, who is also well experienced in uniportal VATS.
Course attendees with Spanish mentoring surgeons:Dr. Maria Delgado (3rd from left), Dr. Mercedes de la Torre (center) and Dr. Ricardo Prado (far right). Dr. Miguel Congregado (first row)
While there have been multiple discussions among STS and other organizations regarding the minimum training required for surgeons to be credentialed and to practice Uniportal VATS and other advanced surgical techniques in their respective hospitals – the wet lab gives no doubt as to the need for ‘hands-on’ experience for even experienced VATS surgeons*.
Lecture content becomes reality
Visiting surgeons during didactic component
Powerpoint discussions, video demonstrations and even the most engaging lectures on bleeding complications quickly take center stage once surgeons enter the lab.
For surgeons who have spent their time watching Dr. Gonzalez Rivas perform a complete lymph node dissection in under 9 minutes, the lab is eye opening.
Despite being cautioned during lectures on preventing and managing bleeding the day before, as well as short review immediately prior to entering the lab, essential pre-operative preparations on surgical trays are noticeably absent in the lab. None of the two man teams takes the time to place spongesticks on their mayo stands or make any other modifications to their instruments prior to making the initial incision.
Attendees experience the reality of bleeding complications during initial attempts at Uniportal VATS
One by one – with two notable exceptions, each of the 8 teams encounters catastrophic bleeding – injuries to the pulmonary arteries, accidental tears to the vena cava and other major problems. But that’s why they are here: to become familiar with uniportal surgery, its specialized instruments while being guided by experienced uniportal VATS surgeons. One by one, the surgeons remember the mantra of Dr. Diego Gonzalez Rivas: “Don’t panic!” as they maneuver and do the best to re-establish hemostasis. Surgeons practice placing stitches in the PA, and repairing the great vessels. All remember the first lesson Uniportal VATS – hold pressure. Some manage these complications quickly with relative ease, others struggle initially and some fail entirely.
Bleeding is not the only possible complication for novice uniportal surgeons
Others, like the pair of general surgeons from the Netherlands demonstrate that despite a steep learning curve, success is possible with uniportal VATS. After initially learning traditional VATS in 2008, these surgeons had just 5 uniportal cases under their belt prior to coming to this course. However, each of their cases were completed quickly and without complications.
The wet lab was followed by a day of live-surgery performed by Dr. Gonzalez Rivas – where attendees could ask questions about his techniques during the operations. Their new found experience in the web lab served as a useful framework for their questions and observations.
*Dr. Gonzalez Rivas and his colleagues recommend attending several courses, followed by a web-lab and then finally, proctoring with an experienced Uniportal VATS surgeon.
Interested in learning uniportal VATS?
Start by familiarizing yourself with the basics – watch YouTube and other surgical demonstration videos like the Virtual VATS uniportal lobectomy on December 3rd 2016, read articles and reviews.
Attend conferences and moderated discussions on the technical aspects of uniportal VATS
Observe ‘live-surgery’ events – like the week long courses at Shanghai Pulmonary Hospital
Attend wet lab courses
Finally, arrange for mini-residencies or mentoring at home facility as you begin to implement these techniques into your own practice. Be prepared to encounter bleeding and other complications and remember: Don’t panic!
Single port thoracoscopic surgery and awake anesthesia: the micro-invasive thoracic surgery? The current research and use of these state of the art techniques to bring minimally invasive surgery to complex surgery and high risk patients.
At a recent high-profile American thoracic surgery conference, one of the speakers presented data from his program showing the safe and effective use of regional and conscious sedation techniques to perform complex thoracic surgery procedures on non-intubated patients.
Instead of being greeted with enthusiasm or professional interest, the great majority of well-known giants in thoracic surgery dismissed the idea with a few, repeated sarcastic, albeit joking remarks about the inconvenience of having conscious patients in the operating room. This attitude seemed perplexing given the results of Pompeo et; al.’s (2014) survey of the European Society of Thoracic Surgeons, in which a large number of respondents (59%) reported using nonintubated thoracic surgery (NITS) procedures. These mixed attitudes led thoracics.org to perform an in-depth literature search to determine the state of non-intubated thoracic surgery.
What is the current status of non-intubated thoracic surgery (and the literature surrounding it)?
Is it a wild, unsustainable idea promoted by a few dynamic but misguided surgeons? Is it a well-researched and promising developing technique that is being rejected by surgeons who may lack vision? Or does it fall into that gray area where we suspect that this technique has real value and benefits for a special subset of patients but there isn’t quite enough high level clinical evidence to demonstrate that to the surgical community?
Is non-intubated thoracic surgery destined to fall to the same fate of VATS – a game-changing technique that emerged in the early 1990’s, has been clinically demonstrated to be superior to open surgery with an overwhelming preponderance of evidence, but still being discussed by many surgeons as the ‘new kid on the block’**? Will people still debate the merits of non-intubated surgery ad infinitude thirty years from now, even when clinical guidelines have made it the standard of care (like VATS and oncology surgery)? Will there be the same reluctance to set firm standards for training in these techniques?
“Not a new concept”
photo courtesy of the US Army
As it turns out – non-intubated thoracic surgery is not a new idea or concept. It was developed early in the 20th century and was used successfully for many years for even the most complex thoracic cases such as esophagectomies until the development of double lumen intubation in the 1950’s made the use of single lung ventilation possible (Gonzalez-Rivas et. al. 2015, Pompeo 2015, Kiss & Castillo 2015). Since its rediscovery in the last several years, many of the problems that plagued this technique during its inception over a century ago have been addressed through better understanding of human physiology. Now, this seemingly fringe technique has been shown to be a feasible approach for treating the very margins of the thoracic surgery population (the extreme elderly, patients with advanced respiratory disease or other serious medical co-morbidities) that are often deemed inoperable using current techniques.
The dreaded complication (spontaneous pneumothorax) of early use of this technique by pioneers in thoracic surgery has now become one of the main advantages. Surgically created pneumothorax results in almost perfect deflation of the operative lung, achieving better results than even the most experienced of anesthesiologists using traditional single lung ventilation. Surprisingly to many observers, instead of creating a ventilatory emergency, this process is readily tolerated by most patients, even those with poor baseline pulmonary function (David, Pompeo, Fabbi & Dauri, 2015).
Current research
The majority of the current series of research on this topic are being performed by a small group of surgeons which includes Dr. Diego Gonzalez Rivas (Spain), Dr. Eugenio Pompeo and the Awake Thoracic Surgery Research Group in Italy and Dr. Ming-Hui Hung and colleagues (Taiwan). Pompeo’s group (Drs Benedetto Cristino, Augusto Orlandi, Umberto Tarantino, Tiziana Frittelli (General Director of the Policlinico Tor Vergata), Leonardo Palombi, Paola Rogliani, Roberto Massa, Mario Dauri) has been especially prolific in 2015 after several of their works were published in a special issue of Annals of Translational Medicine.
In multiple studies, these researchers have reported successful thoracic surgery outcomes in non-intubated patients, thus eliminating the majority of risks related to general anesthesia as well as uni-lung ventilation via mechanical ventilation and intubation. In several of these studies, the authors were also able to successfully perform these surgeries in fully awake patients (versus consciously sedated), making surgery possible for even the frailest of candidates. These studies included a small number of comparisons between traditional and non-intubated surgeries. While the numbers of patients enrolled have been small, and there are few randomized studies, the results have been encouraging.
Chen et. al
Chen et. al’s 2012 study has been one of the largest studies to date, with 285 cases. In this study, patients underwent lobectomies, wedge resections and segmentectomies with 4.9% requiring conversion with tracheal intubation. Lung resection was undertaken with traditional (3 port) VATS or a needlescopic approach.
The authors report the biggest problem they encountered was increased bronchial tone and airway hyper-reactivity during manipulation of the pulmonary hilum during lobectomies and segmentectomies. This was effectively treated without significant alteration in hemodynamics via intrathoracic vagal blockage which eliminated the cough reflex in these patients.
The authors caution judicious patient selection to prevent emergent conversion (intubation) particularly while surgeons are initially attempting this technique. Chen et al. also believe that non-intubated thoracic surgery is best suited for petite or small-sized female patients because the small tracheal size of these patients predisposes them to a higher rate of complications and potential tracheal injury with traditional surgery and intubation.
Awake anesthesia and lung volume reduction surgery
Pompeo et. al’s review of the literature surrounding of the use of this technique in patients with severe emphysema undergoing nonresectional lung volume reduction surgery (LVRS by awake anesthesia) showed significant treatment advantages for patients undergoing lung volume reduction surgery without intubation or administration of general anesthesia.
With an average mortality of 5% and a morbidity of 59% for traditional lung volume reduction surgery as reported during the National Emphysema Treatment Trial, findings from Tacconi et al.’s 2009 study of 66 LVRS awake patients (matched with 66 patients undergoing traditional surgery) appears promising. The authors report a reduced incidence of prolonged air leaks (18%) versus 40% in the traditional surgical group as well as a decreased length of stay. In this study, 3 patients required conversion to general anesthesia – one patient due to an elevated paCo2 of 83% and the remaining two patients for anxiety attacks.
Rate of intubation/ respiratory failure/ mortality in Tacconi et al.
Mortality in both non-intubated and the traditional surgical group was the same, with one patient from each group. In both cases, the patients had developed massive airleaks following surgery. In the non-intubated group, the patient developed acute lung injury requiring intubation of POD#12 and died POD#38.
In the traditional surgical group, 4 patients were unable to be extubated at the end of the case, with one patient requiring an additional day of mechanical ventilation. Another patient was reintubated on POD#3 for respiratory failure and died on POD#67.
Pompeo et. al, over the course of over eleven years, have also investigated the use of non-intubated (and awake) thoracic surgery for a wide variety of cases including urgent /emergent cases, wedge resections, decortications, talc pleurodesis as well as nonintubated anesthesia combined with single (uniportal) thoracoscopic approaches (aka “microinvasive thoracic surgery”).
Anesthesia for non-intubated thoracic surgery
The role of anesthesiologists in caring for patients undergoing non-intubated or awake thoracic surgery is more challenging than general anesthesia. While thoracic anesthesia already requires specialized skills for initiating, managing and maintaining uni-lung ventilation, the switch to non-intubated patients with either localized anesthesia or conscious sedation adds a new set of complexity to managing these often frail patients. Kiss & Castillo (2015) in their review of the literature, provide an excellent overview of the pros and cons of non-intubated anesthesia as well as guidelines for patient selection and eligibility criteria for use of this technique. Special populations who may benefit from this technique include patients with severe respiratory disease (and a high risk of ventilator dependency with intubation), patients with severe but stable dyspnea, or multiple cardiovascular and respiratory co-morbidities.
Kiss et. al also reviews the contraindications to use of this technique including: phrenic nerve paralysis on the non-operative side, patients at risk for difficult intubation, or patients who are unwilling to undergo awake thoracic surgery. Wang & Ge (2014) expand on these complications to include ASA status 4 or higher, bleeding disorders, decompensated heart failure, extreme obesity, unfavorable airway or spinal anatomy as well as specific respiratory conditions including bronchiestasis, asthma, sleep apnea, clinically significant sputum production and strict contralateral lung isolation.
Wang & Ge also give specific anesthesia dosing guidelines for conscious sedation, local anesthesia and regional blocks in additional to monitoring parameters.
Alterations in oxygenation and ventilation
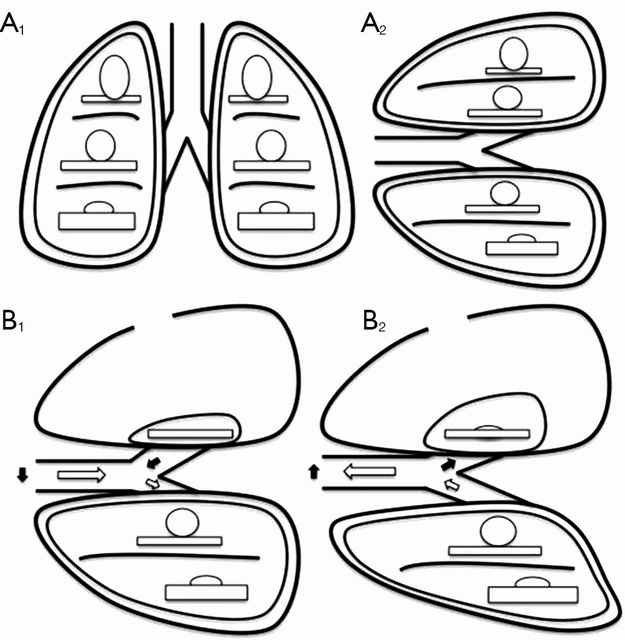
David et. al. (2015) describe the pathophysiology and alterations in oxygenation and ventilation in surgical pneumothorax including hypercapnia, hypoxia and the associated hypoxic pulmonary vasoconstriction that occurs along with the development of intrapulmonary shunt as the deflated (and unventilated lung) maintains perfusion. The authors also explain how this effect can be either exacerbated or minimized thru the choice of anesthetic agents, and the administration of supplemental oxygen, which further demonstrates the importance of involving the thoracic anesthesia team in preparation for non-intubated cases.
The relationship between ventilation and perfusion. (A) Relationship between ventilation (roundes) and perfusion (rectangles) in different lung zones, in upright (A1) and lateral position (A2); (B) relationship between ventilation (roundes) and perfusion (rectangles) in lateral position with surgical pneumothorax, during spontaneous inspiration (B1) and exhalation phase (B2). Black arrows show paradoxical ventilation and mediastinal shift. (Illustration and caption from David et. al, 2015)
This “permissive hypercapnia” has been reported in multiple articles as having minimal to no clinical effects and is easily treated with supplemental oxygen by nasal cannula or facemask.
Editor’s note: In advance of this article, Dr. Pompeo, Dr. Gonzalez Rivas and Dr. Min-Hui Hung were contacted for their additional comments and insights on non-intubated thoracic surgery. This and subsequent articles may be augmented, as applicable with their replies.
Conclusion
Should we really abandon pursuit of better patient outcomes, faster mobility, recovery and reduced length of stay in lieu of the security to tell off-color jokes with our patients safely under general anesthesia? Should we abandon all hope in treating patients previously deemed inoperable due to our own fears and hesitations to embrace newer techniques and procedures?
Or as Mineo et al, suggests, should we enlist our colleagues to design and devise several large scale studies at multiple institutions so that we can move to the next level of investigation and answer the question: “Should my patient be awake for this?”
Mineo TC, Tacconi F. (2014). Nonintubatedthoracic surgery: a lead role or just a walk on part?Chin J Cancer Res. 2014 Oct;26(5):507-10. doi: 10.3978/j.issn.1000-9604.2014.08.11. No abstract available. Very enjoyable, almost conversational article with the authors sharing their experiences with non-intubated thoracic surgery while calling for larger clinical research studies on the topic.
Pompeo, E. (2015). Non-intubated thoracic surgery: nostalgic or reasonable? Annals of Translational Medicine, 2015; 3(8): 99. Review of the historical development on non-intubated thoracic surgery and techniques in regional anesthesia for complicated thoracic surgery procedures including esophagectomies in the era predating the development of double lumen intubated and unilung ventilation. A timely reminder that some of the greatest developments in medicine and surgery are ‘rediscoveries’ of our predecessors.
Pompeo E; Awake Thoracic Surgery Research Group (2012). To be awake, or not to be awake, that is the question. J Thorac Cardiovasc Surg. 2012 Jul;144(1):281-2; author reply 282. doi: 10.1016/j.jtcvs.2012.01.083. No abstract available. Comment on article by Noda et. al.
Note: This is not an exhaustive list of literature available on this topic but a select listing of the most recent and relevant citations (and are available as free full text).
**Long time readers of thoracics.org may have noticed that we no long cover or report on ‘debates’ or discussions as to whether VATS can be used in oncology cases, or whether an adequate lymph node dissection can be performed using VATS. The literature clearly demonstrates that it can – and clinical guidelines reflect this, making the discussion one-sided, tedious, out-dated and repetitious.
Dr. Diego Gonzalez Rivas discusses intubated and nonintubated uniportal thoracic surgery for complex thoracic procedures
Orlando, Florida
Dr. Diego Gonzalez Rivas discusses non-intubated thoracic surgery
One of the standout presentations on Day One of the Duke Masters of Minimally Invasive Thoracic Surgery was Dr. Diego Gonzalez Rivas’ presentation on performing uniportal surgery on non-intubated patients. Surprisingly, this presentation was greeted with significant skepticism in the form of comments by fellow presenters.
No trocars, no rib spreading, one incision (with no rigid port placement)
The use of one small 2.5 cm incision with the camera placed above the instruments allows the surgeon to maintain the traditional perspective of open surgery using a minimally invasive approach. “Eyes above hands” Dr. Gonzalez states, reminding surgeons how to keep their visual perspective unaltered. He also discussed some of the findings from an upcoming 2016 paper [in-press] entitled, “Pushing the envelope” which reviews the developments in the areas of single port (uniportal) thoracic surgery in non-intubated patients. This along with his new textbook, have dominated the international thoracic surgery news in recent years.
As part of his discussion, he demonstrated the ease and feasibility of performing a complete and thorough lymph node dissection using the uniportal approach.
Complete paratracheal lymph node dissection in a non-intubated patient
He also presented several complex thoracic cases such as a bronchial sleeve resection for carcinoid tumor in a young, otherwise healthy female, as well as a double sleeve case, and a uniportal bronchovascular reconstruction. He discussed distal tracheal resection using high frequency ventilation jet in a non-intubated patient after resecting the carina – tracheal anastamosis and several chest wall resection cases via the uniportal approach. But the main portion of his talk was devoted to the specifics of non-intubated surgery – from anesthesia protocols to creating a anatomic (surgical) pneumothorax which eliminates problems of lung inflation during surgery. He discussed that while totally awake nonintubated surgery can be performed (with patients awake and talking), that he prefers the use of conscious sedation for patient comfort.
Nonintubated patient – VATS lobectomy
He highlighted the benefits of these approaches – with non-intubated surgical techniques allowing surgeons to operate on frailer, sicker patients who might otherwise be ineligible for surgery. He also talked about the benefits of uniportal surgery versus robotic surgery. Uniportal surgery is faster, and cheaper than costly robotic techniques that require lengthy patient positioning as well as the use of robotic tools that have to be replaced after 10 to 20 cases.
He also reviewed the relative contraindications for nonintubated surgery:
obese patients (BMI greater than 35)
patients with Malpati scores of 3 or 4 (difficult to intubate patients – in case of the need for emergent intubation)
patients with pulmonary hypertension (who will not tolerate permissive hypercapnia)
Masses greater than 6 cm in size
But he also reminded attendees that relative contraindications often change in the face of more experience.
information about the upcoming VATS symposium in Cambridge, UK – with featured speakers Dr. Diego Gonzalez Rivas and Ian Hunt.
Another conference/ educational announcement for all residents, fellows and interested thoracic surgeons. This course is sponsored by the United Kingdom’s National Health Service and is being held in Cambridge, UK at Papworth Hospital this November. There is parallel content for nurses and other thoracic surgery personnel.
Internationally known Spanish surgeon Dr. Diego Gonzalez Rivas as well as native surgeon Mr. (Dr.) Ian Hunt of St. George’s Hospital in London, will be part of the faculty teaching this course.
Dr. Gonzalez Rivas will be discussing single port surgery in addition to performing a live case on the second day of the symposium.
Mr. Hunt will be discussing how to perform a total lymphadenectomy, as well as lymphadenectomies on more complicated cases.
Additional speakers will be discussing topics including issues in thoracic anesthesia, management of bleeding (in VATS and other minimally invasive surgery), and managing other operative complications.
the latest from Dr. Diego Gonzalez Rivas and the masters of thoracic surgery.
Dr. Gonzalez Rivas and the Thoracic Surgery Unit in Coruna, Spain are hosting the “International Symposium on Uniportal VATS” this week (February 26th to 28th, 2014).
Dr. Gonzalez Rivas demonstrates uniportal VATS
While the in-person, on-site event is limited to just 100 attendees, the event will be offering real-time live streaming surgery for viewers worldwide.
With registrations from around the world, Dr. Gonzalez Rivas estimates that thousands of pairs of eyes will be watching; from Australia to Saudi Arabia, Hong Kong to Colombia, Brazil to Russia, and the United States.
If you’ve ever wanted to learn more about single port VATS, this is the time to find out.
For more information:
Livethoracic.com – link to the event and on-line registration. Registration is 500 Euros.
Article at Examiner.com with more details on this event.
a report from Dr. Chin Hao Chen and his colleagues at Mackay Memorial Hospital on 21 cases of diaphragmatic plication via single and dual port thoracoscopy.
Dr. Chen and his colleagues at Mackay Memorial Hospital in Taiwan published a new article on their experiences using single and dual port thoracoscopy for diaphragm plication.
The report follows 21 cases from July of 2008 to December of 2011. All 21 cases with left-sided eventrations. 11 were plicated using dual port thoracoscopy in the time period prior to January 2010. In January of 2010, single port thoracoscopy became routine practice at Mackay Memorial. The 10 subsequent cases were all performed by single-port thoracoscopy.
Surgical procedure: The average surgical time between dual port and single port varied by ten minutes with dual port surgery taking longer, averaging 92 minutes. ( see Table 1 of original article). 2.0 silk suture was used for plication of the diaphragm.
Port placement:
In cases using dual port thoracoscopy, the surgeons made the first port at the 7th ICS near the MCL with a second port at the 4th or 5th ICS along the anterior axillary line.
For single port cases, the sole port was 1.5 to 2.0 cm in length and was placed at the 6th ICS along the anterior axillary line.
Example of sutured diaphragm – (view from thoracotomy) Photo courtesy of Dr. Ochoa, 2012.
At the conclusion of the VATS procedure for all patients, a single 24fr or 28fr chest tube was placed, and marcaine was administered as a intercostal block. Patients were extubated prior to leaving the operating room.
The chest tube was removed on the first or second post-operative day. Patients were discharged home following chest tube removal. Post-operative pain scores were minimal, and there was no operative mortality.
The authors discuss surgical technique, and port location for a significant portion of the article. Interested readers are advised to read the original for more details.
Discussion:
Interestingly, while much of the literature on diaphragmatic eventration focuses on early repairs of this condition (neonates and pediatric cases), all of the patients in this series were adults, with an average age of 54 – 55 years of age. Both genders were represented; 15 women and 6 men, with an almost equal distribution among single and dual port cases. (3 men in each group, 7 women in single port, 8 in dual port.)
Unlike traumatic diaphragmatic tear or rupture, diaphragmatic eventration is usually a congenital condition and may be asymptomatic. It is often discovered incidentally after patients undergo radiographic studies for other conditions. However, this condition may predispose patients to other conditions such as respiratory distress or dyspnea by compromising respiratory function on the affected side. In fact, the affected lung may appear tiny, and underdeveloped at the time of repair.
In Dr. Wu and Dr. Chen’s study, patients who underwent dual or single port thoracoscopy reported pain scores of four or less at 24 and 36 hours post-operatively. Post-operative hospitalization was short, with patients being discharged on the first or second post-operative day, with no recurrences or mortality.
Reference Article:
Hsin-Hung Wu, Chih-Hao Chen, Ho Chang, Hung-Chang Liu, Tzu-Ti Hung and Shih-Yi Lee (2013). A preliminary report on the feasibility of single-port thoracoscopic surgery for diaphragm plication in the treatment of diaphragm eventration. Journal of Cardiothoracic Surgery 2013, 8:224. Provisional pdf of free full text article, with radiographs, color photographs.
Some of the biggest names in thoracic surgery were in attendance, to present their research and surgical techniques to a crowd of over 600 Chinese thoracic surgeons. The lectures (and live surgery) were also broadcast across China.
World-renown thoracic surgeons at the 16th National Forum in Shanghai, China
Invited International Speakers included:
Dr. G. Alexander Patterson, thoracic surgeon/ lung transplant from the Washington School of Medicine in St. Louis, Mo. (USA). Dr. Patterson gave a lecture on clinical experiences and advances in Lung Transplantation. He also lectured on pancoast tumors.
Dr. Claude Deschamps, French Canadian thoracic surgeon and Chair of Surgery at the Mayo Clinic, Rochester, MN (USA). Dr. Deschamps talked about the use of anti-reflux surgery.
Dr. Gaetano Rocco, of the National Cancer Institute in Naples, Italy. Dr. Rocco talked about advances in chest wall reconstruction. He gave another lecture on uniport surgery.
Dr. Alan Sihoe from the University of Hong Kong discussed management of air leaks.
Surgeons from Taiwan and mainland China presented on a variety of topics including tracheal surgery, management of empyema, sympathectomy for hyperhidrosis and surgical treatment of tuberculosis. (The full list of speakers and topics presented is available here*.)
Conference Spotlight: Single port surgery
But the focal point of the forum was single port (uniportal) surgery. Saturday (the 19th) was devoted to lectures and demonstrations of the single port thoracoscopic technique, including live surgical demonstrations performed by Dr. Diego Gonzalez Rivas. His live surgery presentation was viewed by 500 surgeons at the conference as well as hundreds of other surgeons via a live feed.
Dr. Gonzalez Rivas demonstrates the single port (uniport) technique in Shanghai, China
Thank you to Dr. Gonzalez Rivas for his submission. We welcome reports, photographs and discussions on recent and upcoming thoracic surgery conferences. If you have a meeting, paper or presentation to share, please contact us at k.eckland@gmail.com
*Information is translated from Mandarin using google software with some obvious translational errors, particularly names of several of the Chinese surgeons.
Dr. Chin Hao Chen revisits one of the basic procedures in thoracic surgery: Chest tube placement
Even Hippocrates placed chest tubes or the history of tube thoracostomy
Chest tube placement has been performed since ancient Greek times. Early physicians, including Hippocrates himself, performed (and wrote about) the use of tube thoracostomy for the treatment of lung abscesses and empyema. Often this procedure is performed using a ‘blind approach’ based entirely on external anatomic features (intercostal spaces) and a fundamental knowledge of internal and chest wall anatomy. Over the years, surgeons have developed guidelines to this technique using palpation/ and other tactile information but none of these techniques challenged initial insertion technique.
With any blind procedure, there is a risk of inadvertent injury due to the lack of visualization, particularly in patients with previous thoracic procedures or infections (adhesions), or when performed by less experienced staff.
Direct visualization during this procedure (akin to VATS) may lessen this risk. However, little has been published on alternatives to the traditional technique.
VGTT: video-guided tube thoracostomy
Our latest post comes directly from Dr. Chih-Hao Chen at Mackay Memorial Hospital in Taiwan.
Dr. Chen presents a video clip demonstrating video-guided tube thoracostomy (VGTT), a technique used to avoid tube-related injury during the course of tube thoracostomy (versus blind insertion). This visualization technique is helpful particularly when performed by inexperienced staff, such as residents or in emergent situations.
A complete description of this technique was recently published in the Annals of Thoracic Surgery.
This paper describes the technique as well as discussing the clinical experience of Dr. Chen and his team in applying this technique to several patients.
Dr. Chin-Hao Chen is a thoracic surgeon at Mackay Memorial Hospital in Taiwan. Dr. Chen is a frequent and valued contributor here at Cirugia de Torax. He has provided several case studies as well as articles and videos on surgical techniques.
in the operating room with Dr. Diego Gonzalez Rivas for single port thoracoscopic (uniportal) surgery.
Hilar mass resection using single port thoracoscopy with Dr. Diego Gonzalez – Rivas
K. Eckland & Andres M. Neira, MD
Instituto Nacional de Cancerlogia
Bogota, Colombia
Surgeon(s): Dr. Diego Gonzalez Rivas and Dr. Ricardo Buitrago
Dr. Diego Gonzalez Rivas demonstrates single port thoracoscopy
Case History:
59-year-old female with past medical history significant for recurrent mediastinal mass previously resectioned via right VATS. Additional past medical history included prior right-sided nephrectomy.
Pre-operative labs:
CBC: WBC 7230 Neu 73% Hgb:14.1 Hct 37 platelets 365000
Pt 12.1 / INR1.1 PTT: 28.3
Diagnostics:
Pre-operative CT scan: chest
edited to preserve patient privacy
Procedure: Single port thoracoscopy with resection of mediastinal mass and lymph node sampling
After review of relevant patient history including radiographs, patient was positioned for a right-sided procedure. After being prepped, and draped, surgery procedure in sterile fashion. A linear incision was made in the anterior chest – mid clavicular line at approximately the fifth intercostal space. A 10mm port was briefly inserted and the chest cavity inspected. The port was then removed, and the incision was expanded by an additional centimeter to allow for the passage of multiple instruments; including camera, grasper and suction catheter.
Dr. Gonzalez Rivas and Dr. Ricardo Buitrago at National Cancer Institute
The chest cavity, pleura and lung were inspected. The medial mediastinal mass was then identified.
As previously indicated on pre-operative CT scan, the mass was located adjacent and adherent to the vessels of the hilum. This area was carefully dissected free, in a painstaking fashion. After freeing the mediastinal mass from the hilum, the remaining surfaces of the mass were resected. The mass was fixed to the artery pulmonary and infiltrating it) . The mass was removed en-bloc. Care was then taken to identify, and sample the adjacent lymph nodes which were located at stations (4, 7 and 10).
Following removal of the tumor and lymph nodes, the area was re-inspected, and the lung was re-inflated. A 28 french chest tube was inserted in the original incision, with suturing of the fascia, subcutaneous and skin layers.
closing the single port incision
Hemostasis was maintained during the procedure with minimal blood loss.
Patient was hemodynamically stable throughout the case, and maintained appropriate oxygen saturations. Following surgery, the patient was awakened, extubated and transferred to the surgical intensive care unit.
Post-operative: Post-operative chest x-ray confirmed appropriate chest tube placement and no significant bleeding or pneumothorax.
Immediate post-operative film (chest tube visible)
Patient did well post-operatively. Chest tube was discontinued on POD#2 and discharged home.
PA & LAT films on post-operative day 2
Discussion: Since the initial published reports of single-port thoracoscopy, this procedure has been applied to an increasing range of cases. Dr. Gonzalez and his team have published reports demonstrating the safety and utility of the single-port technique for multiple procedures including lobectomies, sleeve resections, segmentectomies, pneumonectomies and mediastinal mass resections. Dr. Hanao Chen (Taiwan) has reported several successful esophagectomies using this technical, as well as bilateral pleural drainage using a unilateral single-port approach.
Contrary to popular perception, the use of a single-port versus traditional VATS procedures (three or more) is actually associated with better visibility and accessibility for surgeons. Surgeons using this technical have also reported better ergonomics with less operating fatigue related to awkward body positioning while operating.
The learn curve for this surgical approach is less than anticipated due to the reasons cited above, and has been cited at 5 to 20 cases by Dr. Gonzalez, the creator of this approach.
The main limitations for surgeons using this technique is often related to anticipated (but potentially unrealized) fears regarding the need for urgent conversion to open thoracotomy. In reality, many of the complications that may lead to urgent conversion, such as major bleeding, are manageable thoracoscopically once surgeons are experienced and comfortable with this approach.
Dr. Gonzalez and his colleagues have reported a conversion rate of less than 1% in their practice. Subsequent reports by Dr. Gonzalez and his colleagues have documented these findings.
Other barriers to adoption of this technique are surgeon-based, and may be related to the individual surgeon’s willingness or reluctance to adopt new techniques and technology. Many of these surgeons would be surprised by how this technique mimics open surgery.
The successful adoption of this technique by numerous thoracic surgery fellows shows the feasibility and ease of learning single-port thoracoscopy by surgeons interested in adopting and advancing their surgical proficiency in minimally invasive surgery.
The benefits for utilizing this technique include decreased length of stay, decreased patient discomfort and greater patient satisfaction.
References/ Additional Readings
Bertolaccini, L., Rocco, G., Viti, A. & Terzi, A. (2013). Surgical technique: Geometrical characteristics of uniportal VATS. J. Thorac Dis. 2013, Apr 07. Article from thoracic surgeons at the National Cancer Institute in Naples, Italy explains how the geometric advantages of uniportal VATS improves visibility and spatial perception over traditional VATS, and mimics open surgery.
Calvin, S. H. Ng (2013). Uniportal VATS in Asia. J Thorac Dis 2013 Jun 20. Article discussing the spread of uniportal techniques in Taiwan, China and other parts of Asia.
Chen, Chin-Hao, Lin, Wei-Sha, Chang, Ho, Lee, Shih-Yi, Tzu-Ti, Hung & Tai, Chih-Yin (2013). Treatment of bilateral empyema thoracis using unilateral single-port thoracoscopic approach. Ann Thorac Cardiovasc Surg 2013.
Gonzalez Rivas, D., Fieira, E., Delgado, M., Mendez, L., Fernandez, R. & De la Torre, M. (2013). Surgical technique: Uniportal video-assisted thoracoscopic lobectomy. J. Thorac Dis. 2013 July 4.
Gonzalez Rivas, D., Delgado, M., Fieira, E., Mendez, L. Fernandez, R. & De la Torre, M. (2013). Surgical technique: Uniportal video-assisted thoracoscopic pneumonectomy. J. Thorac Dis. 2013 July 4.
Rocco, G. (2013). VATS and uniportal VATS: a glimpse into the future. J. Thorac Dis. 2013 July 04. After coming across several articles by Dr. Gaetano Rocco, and actively pursuing several other publications by this Italian thoracic surgeon, I have become increasingly convinced that Gaetano Rocco, along with Dr. Gonzalez Rivas is one of the world’s leading innovators in thoracic surgery. Hopefully, cirugia de torax will be able to catch up to Dr. Rocco at some point for an in-depth discussion.
Rocco G. Single port video-assisted thoracic surgery (uniportal) in the routine general thoracic surgical practice. Op Tech (Society of Thoracic and Cardiovascular Surgeons). 2009;14:326–335.
Rocco G, Khalil M, Jutley R. Uniportal video-assisted thoracoscopic surgery wedge lung biopsy in the diagnosis of interstitial lung diseases. J Thorac Cardiovasc Surg. 2005;129:947–948.
5 / Video-assisted thoracic surgery lobectomy: 3-year initial experience with 200 cases. Gonzalez D, De la Torre M, Paradela M, Fernandez R, Delgado M, Garcia J,Fieira E, Mendez L. Eur J Cardiothorac Surg. 2011 40(1):e21-8.
6 / Single-port Video-Assisted Thoracoscopic Anatomical Resection: Initial Experience. Diego Gonzalez , Ricardo Fernandez, Mercedes De La Torre, Maria Delgado, Marina Paradela, Lucia Mendez. Innovations.Vol 6.Number 3. May/jun 2011. Page 165.
the 2013 S.W.A.T conference, presented by Johnson & Johnson. Featured presenters Dr. Diego Gonzalez Rivas and Dr. Paula Ugalde discuss single port thoracoscopy and topics in minimally invasive surgery
Very pleased that despite the initial difficulties, we are able to provide information regarding the recent conference.
Talking about Single-port surgery in Bogotá, Colombia – 2013 S.W.A.T. Summit
Dr. Diego Gonzalez Rivas and Dr. Paula Ugalde were the headliners at the recent Johnson and Johnson thoracic surgery summit on minimally invasive surgery. Both surgeons gave multiple presentations on several topics. They were joined at the lectern by several local Colombian surgeons including Dr. Stella Martinez Jaramillo (Bogotá), Dr. Luis Fernando Rueda (Barranquilla), Dr. Jose Maineri (Venezuela) Dr. Mario Lopez (Bogotá) and Dr. Pardo (Cartagena).
Thoracic surgeons at the 2013 S.W.A.T Summit in Bogota, Colombia. Drs. Gonzalez-Rivas and Dr. Paula Ugalde are center, front-row
Target audience missing from conference
The audience was made up of thirty Latin American surgeons from Colombia, Costa Rica and Venezuela. This surgeons were hand-picked for this invitation-only event. Unfortunately, while Johnson and Johnson organized and presented a lovely event; their apparent lack of knowledge about the local (Colombian) thoracic surgery community resulted in the exclusion of several key surgeons including Dr. Mauricio Velasquez, one of Colombia’s earliest adopters of single-port thoracoscopy. Also excluded were the junior members of the community, including Dr. Castano, Dr. Carlos Carvajal, and current thoracic surgery fellows. It was an otherwise outstandingand informative event.
The Gonzalez – Rivas dissector, photo courtesy of Scanlon International
As discussed in multiple publications, previous posts as well as during the conference itself, it is these younger members who are more likely to adopt newer surgical techniques versus older, more experienced surgeons. More seasoned surgeons may be hesitant to change their practices since they are more comfortable and accustomed to open surgical procedures.
Despite their absence, it was an engaging and interesting conference which engendered lively discussion among the surgeons present.
Of course, the highlight of the conference actually occurred the day before, when Dr. Gonzalez- Rivas demonstrated his technique during two separate cases at the National Cancer Institute in Bogotá, Colombia. (Case report).
Dr. Gonzalez-Rivas and Dr. Ricardo Buitrago performing single port thoracoscopy at the National Cancer Institute
Featured presenters:
Dr. Diego Gonzalez – Rivas is a world-renown thoracic surgeon jointly credited (along with Dr. Gaetano Rocco) with the development of single-port thoracoscopic (uni-port) surgery. He and his colleagues at the Minimally Invasive Surgery Unit in La Coruna, Spain give classes and lectures on this technique internationally. Recent publications include three papers in July alone detailing the application of this surgical approach, as well as several YouTube videos demonstrating use of this technique for a wide variety of cases.
Dr. Gonzalez Rivas
Dr. Paula Ugalde, a Chilean-borne thoracic surgeon (from Brazil) who gave several presentations on minimally-invasive surgery topics. She is currently affiliated with a facility in Quebec, Canada.
Dr. Paula Ugalde
Refuting the folklore
Part of the conference focused on refuting the ‘folklore’ of minimally-invasive procedures. Some of these falsehoods have plagued minimally-invasive surgery since the beginning of VATS (in 1991), such as the belief that VATS should not be applied in oncology cases. The presenters also discussed how uniportal VATS actually provides improved visibility and spatial perception over traditional VATS (Bertolaccini et al. 2013).
However, Gonzalez-Rivas, Ugalde and the other surgeons in attendance presented a wealth of data, and publications to demonstrate:
– VATS is safe and feasible for surgical resection in patients with cancer. (Like all surgeries, oncological principles like obtaining clear margins, and performing a thorough lymph node dissection need to be maintained).
– Thorough and complete lymph node dissection is possible using minimally invasive techniques like single-port surgery. Multiple studies have demonstrated that on average, surgeons using this technique obtain more nodes than surgeons using more traditional methods.
– Large surgeries like pneumonectomies and sleeve resections are reasonable and feasible to perform with single-port thoracoscopy. Using these techniques may reduce morbidity, pain and length of stay in these patients.
– Rates of conversion to open surgery are very low (rare occurrence). In single-port surgery, “conversion” usually means adding another port – not making a larger incision.
– Learning curve fallacies: the learning curve varies with each individual surgeon – but in general, surgeons proficient in traditional VATS and younger surgeons (the “X box generation”) will readily adapt to single-port surgery.
– Bleeding, even significant bleeding can be managed using single-port thoracoscopy. Dr. Gonzalez Rivas gave a separate presentation using several operative videos to demonstrate methods of controlling bleeding during single-port surgery – since this is a common concern among surgeons hesitant to apply these advanced surgical techniques.
Additional References / Readings about Single-Port Thoracoscopy
Scanlon single-port thoracoscopy kits – informational brochure about specially designed instruments endorsed by Dr. Gonzalez Rivas.
Dr. Diego Gonzalez Rivas – YouTube channel : Dr. Gonzalez Rivas maintains an active YouTube channel with multiple videos demonstrating his surgical technique during a variety of cases. Below is a full-length video demonstrating the uniportal technique.
Additional posts at Cirugia de Torax about Dr. Diego Gonzalez- Rivas
Upcoming conference in Florida – information about registering for September conference for hands-on course in single-port thoracoscopic surgery with Dr. Gonzalez-Rivas
Youtube video for web conference on Single-port thoracoscopic surgery
Bertolaccini, L., Rocco, G., Viti, A. & Terzi, A. (2013). Surgical technique: Geometrical characteristics of uniportal VATS. J. Thorac Dis. 2013, Apr 07. Article from thoracic surgeons at the National Cancer Institute in Naples, Italy explains how the geometric advantages of uniportal VATS improves visibility and spatial perception over traditional VATS, and mimics open surgery.
Calvin, S. H. Ng (2013). Uniportal VATS in Asia.J Thorac Dis 2013 Jun 20. Article discussing the spread of uniportal techniques in Taiwan, China and other parts of Asia.
Rocco, G. (2013). VATS and uniportal VATS: a glimpse into the future.J. Thorac Dis. 2013 July 04. After coming across several articles by Dr. Gaetano Rocco, and actively pursuing several other publications by this Italian thoracic surgeon, I have become increasingly convinced that Gaetano Rocco, along with Dr. Gonzalez Rivas is one of the world’s leading innovators in thoracic surgery. Hopefully, cirugia de torax will be able to catch up to Dr. Rocco at some point for an in-depth discussion.
While I advance criticism of this event – it was a fantastic conference. My only reservations were to the exclusivity of the event. While this was certainly related to the costs of providing facilities and services for this event – hopefully, the next J & J thoracic event will be open to more interested individuals including young surgeons and nurses.
Reviewing “Ten years experience on 644 patients undergoing single-port (uniportal) video-assisted” by Gaetano Rocco et al. at the National Cancer Institute in Naples, Italy
In this month’s issue of the Annals of Thoracic Surgery, Dr. Gaetano Rocco and his colleagues at the National Cancer Institute, Pascale Foundation in Naples, Italy reported their findings on ten year’s worth of single-port surgery in their institution.
Who: 644 patients; (334 males, 310 females)
Indications:
Annals of thoracic surgery – Rocco et. al (2013)
What: Outcomes and experiences in single port thoracic surgery over a ten-year period. All procedures performed by a single surgeon at this institution, and single-port VATS accounted for 27.7% of all surgeries performed during this time period.
When: data collected on thoracic surgery patients from January 2000 – December 2010.
Technical Notes:
Pre-operative CT scan was used for incision placement planning. Incision was up to 2.5 cm (1 inch) in length depending on indications for surgery.
Conversion rate to 2 or 3 port VATS: 2.2% (14 patients)
Conversion to mini-thoracotomy: 1.5% (10 patients)
Patients underwent conversion due to incomplete lung collapse (22 patients) and bleeding (2 patients).
There were no re-operations or “take backs”. The four patients with malignant effusions who died within the 30 day post-op period were re-admitted to the ICU.
Post-operatively:
Otherwise, all patients were admitted to either the floor or the step-down unit following surgery.
Pain management: post-operative pain was managed with a non-narcotic regimen consisting of a 24 hour IV infusion pump of ketorolac (20mg) and tramadol (100mg*). After the first 24 hours, patients were managed with oral analgesics such as paracetamol (acetaminophen).
Limitations: in this study, uni-port VATS was not used for major resections, as seen in the work of Dr. Diego Gonzalez and others. This may be due to the fact that uni-port VATS was an emerging technique at the initiation of this study.
Strengths: This is one of the largest studies examining the use of single-port thoracic surgery – and showed low morbidity and mortality. (Arguably, the 30 day mortality in this study was related to the patients’ underlying cancers, rather than the surgical procedure itself.)
*Intravenous tramadol is not available in the United States.
Rocco G. Single port video-assisted thoracic surgery (uniportal) in the routine general thoracic surgical practice. Op Tech (Society of Thoracic and Cardiovascular Surgeons). 2009;14:326–335.
Rocco G, Khalil M, Jutley R. Uniportal video-assisted thoracoscopic surgery wedge lung biopsy in the diagnosis of interstitial lung diseases. J Thorac Cardiovasc Surg. 2005;129:947–948.
What kind of pain should patients expect after thoracic surgery, and how long will it last? Also, is this normal? When should I call my doctor?
Like all posts here at Cirugia de Torax, this should serve as a guide for talking to your healthcare provider, and is not a substitute for medical advice.
Quite a few people have written in with questions about post-operative pain after thoracic surgery procedures so we will try to address those questions here.
1. What is a normal amount of pain after these procedures?
While no two people will experience pain the same, there are some general guidelines to consider. But to talk about this issue – we will need to refer to a basic pain scale which rates pain from 0 (no pain) to 10 – (excruciating, writhing pain, worst possible imaginable).
Unfortunately, for the majority of people who have thoracic surgery, there will be some pain and discomfort.
Pain depends on the procedure
In general, the intensity and duration of pain after thoracic procedures is related to the surgical approach – or the type of surgical incision used.
This open incision (with rib spreading) will hurt more.. Photo: advanced empyema requiring open thoracotomy for decortication
Pain will be much less with a single incision VATS surgery (now with chest tube) and specimen removed (photo courtesy of Dr. Chen)
Patients with larger incisions like a sternotomy, thoracotomy or clamshell incision will have more pain, for a longer period of time than patients that have minimally invasive procedures like VATS because there is more trauma to the surrounding tissues. People with larger incisions (from ‘open surgeries’) are also more likely to develop neuralgia symptoms as they recover.
. (I will post pictures of the various incisions once I return home to my collection of surgical images).
Many patients will require narcotics or strong analgesics for the first few days but most surgeons will try to transition patients to anti-inflammatories after surgery.
Post-operative surgical pain is often related to inflammation and surgical manipulation of the chest wall, particularly in procedures such as pleurodesis, decortication or pleurectomy. For many patients this pain will diminish gradually over time – but lasts about 4 to 6 weeks.
Anti-inflammatories
This pain is often better managed with over the counter medications such as ibuprofen than with stronger narcotics. That’s because the medication helps to relieve the inflammation in addition to relieving pain. Anti-inflammatory medications also avoid the risks of oversedation, drowsiness and severe constipation that often comes with narcotics.
Use with caution
However, even though these medications are available without a prescription be sure to talk to your local pharmacist about dosing because these medications can damage the kidneys. Also, be sure to keep hydrated while taking this medications.
People with high blood pressure should be particularly cautious when taking over the counter anti-inflammatories because many of these medications have drug interactions with blood pressure medications.
2. “I had surgery three weeks ago, and I recently developed a burning sensation near the incision”
Neuralgias after surgery
For many patients, the development of a neuralgia is a temporary effect and is part of the healing process. However, it can be quite disturbing if patients are unprepared. Neuralgic pain is often described as a burning or stinging sensation that extends across the chest wall from the initial incision area. Patients also describe it as a ‘pins and needles’ sensation or “like when your foot falls asleep”. This usually develops a few weeks after surgery as the nerves heal from the surgery itself.
It the discomfort is unmanageable, or persists beyond a few weeks, a return visit to your surgeon is warranted. He/She can prescribe medications like gabapentin which will soothe the irritated nerves and lessen the sensations. However, these medications may take some time to reach full effect.
Range of motion and exercise after surgery
Exercise limitations are related to the type of incision.
Sternotomy incisions/ sternotomy precautions
If you have a sternotomy incision – (an incision through the breast bone at the center of your chest), this incision requires strict precautions to prevent re-injury to the area. Since the sternal bone was cut, patients are usually restricted from lifting anything greater than 10 pounds for 6 to 12 weeks, and to avoid pushing, pulling or placing stress on the incision. Patients are also restricted from driving until bone healing is well underway. (Be sure to attend a rehab program or physical therapy program to learn the proper way to exercise during this time period).
Patients will also need to take care to prevent a surgical skin infection or something more serious like mediastinitis. The includes prohibitions against tub bathing/ soaking, swimming or over- aggressive cleaning of the incision with harsh abrasives like hydrogen peroxide or anti-bacterial soaps. These chemicals actually do more harm than good in most cases by destroying the newly healing tissue. A good rule of thumb to remember (unless your doctor says otherwise): No creams or lotions to your incisions until the scabs fall off.
Post-thoracotomy incisions
With a large thoracotomy incision, most patients will be restricted from lifting any items greater than 10 pounds on the surgery side for around two weeks. However, unlike sternotomy patients – we want you to use and exercise that arm daily – otherwise patients have a risk of developing a ‘disuse’ syndrome. One of the common exercises after a thoracotomy is called the spider crawl. This exercise helps the muscles to heal and prevent long-term disability or problems. The physiotherapist at your local hospital should have a list of several others that they can teach you to practice at home.
The spider crawl
In this example, the patient had a left thoracotomy:
1. Stand with your surgical side within arm’s length of the wall.
start with your hand at waist level
Now, use your hand to “walk” up the wall, similar to a spider crawling.
‘walking’ the hand up the wall
Continue to walk your hand up the wall until your arm is fully extended.
continue until arm fully extended
Perform this exercise (or similar ones) for several minutes 5-6 times a day. As you can see – it is fast and easy to do.
VATS
For patients with minimally invasive procedures – there are very few exercise restrictions, except no heavy lifting for 2 to 3 weeks (this is not the time to help your neighbor move his television.)
General incision care guidelines are similar to that for sternotomy patients – no soaking or bathing (showering is usually okay), no creams or lotions and no anti-bacterial soaps/ hydrogen peroxide/ harsh cleaners.
Whats NOT normal – when it’s time to call your surgeon
– dramatic increase in pain not associated with activity (i.e. lifting or reaching). If your pain has been a “4” for several days and suddenly increases to an “8”
– If the quality of the pain changes – ie. if it was a dull ache and becomes a stabbing pain.
– any breathlessness, shortness of breath or difficulty breathing
– Any increase in redness, or swelling around your incisions. Incisions may be pink and swollen for the first 2-3 days, but any increase after that warrants a ‘wound check’ by your surgeon
– Any fresh bleeding – bright red blood. A small amount of drainage (from chest tube sites) that is light pink, clear or yellow in nature may be normal for the first few days.
– Drainage from the other sites (not chest tube sites) such as your primary incision is not normal and may be a sign of a developing infection.
– Fever, particularly fever greater than 101.5 – may be a sign of an infection.
– If you are diabetic, and your blood sugars become elevated at home, this may also be a sign of infection. (Elevation in the first few days is normal, and is often treated with insulin – particularly if you are in the hospital.
– Pain that persists beyond 3 months may be a sign of nerve damage (and you will need additional medications / therapies).
For thoracic surgeons interested in becoming more familiar with uniport surgery, this is your chance to learn from the pioneers of the technique.
Several new dates for Uni-port thoracoscopy with Dr. Diego Gonzalez Rivas. These events span across the Americas and Europe, so if you are interested in uni-port thoracoscopic surgery, then there is something nearby.
The first date is coming up soon – in August 2013, in Bogotá, Colombia.
Dr. Diego Gonzalez Rivas in Bogotá, Colombia
I am excited about this one, and hope to be able to cover the event for readers of CdeT. While I am currently in Medellin, I became familiar with, (and have a great deal of respect for) many of Bogotá’s finest thoracic surgeons in the past so it’s a great opportunity not just to hear more about Dr. Diego Gonzalez Rivas and uni-port thoracoscopy but to check in local surgeons and hear about some of their more interesting cases.
Dr. Gonzalez will be joined by Dr. Paula Ugalde, a well-known thoracic surgeon from Brazil (now practicing in Quebec, Canada).
As soon as I get some more details on the Bogotá event – I’ll post them here..
Split, Crotia – September 12th – 15th – 23rd Congress of the World Society of Cardio-Thoracic Surgeons.
This conference is being jointly sponsered by the Society of Cardio-Thoracic Surgeons of South Africa (SCTSSA). Dr. Diego Gonzalez will be talking about “Uni-port VATS major pulmonary resections in advanced lung cancer” in an afternoon session on September 13, 2013. (Obviously they don’t know much about him – since it’s only a 20 minute session – but as a CTS conference, only about 10% is thoracic topics (he is one of just a handful of thoracic speakers.)
Then in mid -September 2013, he will part of a roster of the greats of thoracic surgery (Dr. Robert Cefolio, Dr. James Luketich and Dr. Thomas D’Amico) at the Duke Center for Surgical Innovation for a course entitled, “Masters of Minimally Invasive Thoracic Surgery”.
The second event, is a meeting/ conference/ training course in Dr. Gonzalez’s home hospital in Coruna, Spain. The event, “Live Thoracic” will feature ‘live-surgery’ demonstrations and will be streamed for real-time viewing from around the world.
In a side note – I want to thank the nearly 6,000 students, interns, nurses, residents and thoracic surgeons who have downloaded one of my thoracic surgery apps for Android devices.
Dr. Chin-Hao Chen demonstrates ‘ultrafast open tracheostomy.’
“Ultrafast open tracheotomy”
Currently tracheostomy procedures are performed one of two ways; using the traditional surgical (open) method and a percutaneous method.
Both methods have benefits and drawbacks. In open tracheostomy, the primary drawback is the need to transport the patient in the operating room at most hospital facilities. Postoperative bleeding is less frequent in open method. However, postoperative wound infection and poor healing of the stoma in some cases may be troublesome.
As a bedside procedure, percutaneous tracheostomy is rapidly gaining in popularity due to the fast, and relative ease of the procedure. However, it comes with its own set of risks and potential complications such as pneumothorax. As a minimally invasive procedure, the risk of bleeding is minimized, but cases of severe hemorrhage have been reported. The cause of this massive and severe bleeding in percutaneous method is partly due to the lack of delicate dissection of pre-tracheal soft tissues, which led the injury of isthmus of thyroid gland, esophagus, and major vessels in the neck.
In summary, percutaneous method provided a faster approach and less wound infection while having the possibility of severe bleeding complication. Open method takes more time to complete the procedure and risk of wound infection is slightly higher. But open dissection method can minimize unnecessary injury and bleeding.
Several studies comparing the two methods have demonstrated fairly equivalent outcomes. However, ultra-fast open tracheostomy offers another option for patients who may need long-term mechanical ventilation.
The method designed by Dr. Chin-Hao Chen is called “ultra-fast open tracheostomy “.
The procedure usually takes around 4-6 minutes. Dr. Chen reports that he has performed the procedure in over 250 cases (253 cases to date). There have been no bleeding complications; (acute or delayed ). We did have a few minor wound infections. We did have one patient, who had a more severe infection (but the patient’s underlying diagnosis was sepsis and organ failure.)
Dr. Chen states, “I invented the procedure about ten years too late. Prior to that, it might have been very popular. But now that the percutaneous puncture method has been developed, it is not so valuable.”
Dr. Chen previously presented, “A Modified Open Method for Sutureless Tracheostomy” at a conference in Taiwan last year. At that time, he discussed his experiences and outcomes performing the procedure on 108 cases. He reported his average operating time as 5.0 minutes.
Dr. Chen has also provided video clips to demonstrate his procedure, which is simple and fast.
References and Resources
Aaron’s tracheostomy page – site about tracheostomies and tracheostomy care by a nurse, Cynthia Bissell. Good reference information for patients and their families.
Mayo Clinic site – all about surgical tracheostomies. (“Minimally-invasive” aka percutaneous)
Cho YJ. (2012). Percutaneous dilatational tracheostomy. Tuberc Respir Dis (Seoul). 2012 Mar;72(3):261-74. doi: 10.4046/trd.2012.72.3.261. Epub 2012 Mar 31
Durban, C. (2005). Types of tracheostomies. Respiratory Care, 50(4): 488 – 496. Excellent article with historical review of techeostomy techniques.
The article, entitled, “Treatment of bilateral empyema thoracis using unilateral single port approach,” details one of his recent cases and discusses the use of unilateral single port surgery for the treatment of bilateral conditions. (For the uninitiated – that’s one small incision to treat an infection on both sides of the chest.)
Case report: bilateral empyema
In this case report, a 28 year old male presented with dyspnea, sore throat, malaise, fever and weakness. Patient was admitted with a diagnosis of sepsis and started on antibiotics.
Labs showed an elevated WBC count (19,300), C-reactive protein and D-dimer. Subsequent imaging confirmed the presence of pulmonary emboli, and with serial imaging showing worsening bilateral pleural effusions. Thoracic surgery was consulted for definitive treatment.
Dr. Chen discusses this technique, as well as considerations for using this novel approach.
First look at innovative approach
Other that his recent discussions here at Cirugia de Torax, this is the first time that surgery utilizing this technique has been discussed in a medical forum. This represents a ground-breaking advance in thoracoscopic surgery, single port surgery and thoracic surgery as a whole.
Update: Article published June 18, 2013 in the Annals of Thoracic and Cardiovascular Surgery. A pdf of the full article is available.
a clinical case report from Bogota, Colombia – and the work of Dr. Kalyanam Shivkumar, MD, PhD, Director, UCLA Cardiac Arrhythmia Center on treating ventricular arrhythmias with cardiac sympathetic denervation, including an upcoming clinical trial.
Dr. Ricardo Buitrago, Thoracic Surgeon
Dr. Andres Franco, Thoracic Surgeon
K. Eckland, Nurse Practitioner
Clinica Shaio
Bogota, Colombia
Left cardiac sympathetic denervation for uncontrolled ventricular arrhythmias in a young child
Dr. Andres Franco (right) assists Dr. Ricardo Buitrago (left) during VATS cardiac denervation
Case History: The patient, a 9-year-old Hispanic female child had a history of congenital long QT syndrome*, and had her first AICD (automated internal cardiac defibrillator) placed at two months of age, after receiving the initial diagnosis as a neonate.
After several years and multiple medical regimens were unsuccessful in controlling frequent episodes of ventricular tachycardia, the patient had undergone several additional procedures aimed at reducing the incidence of arrhythmia. The device had been checked thoroughly, evaluated and exchanged twice as part of on-going evaluation to ensure that the device was working properly, and was set at appropriate thresholds.
At the time of the initial referral to thoracic surgery, the child suffered from intense post-traumatic stress disorder symptoms and was being treated for psychiatric disturbances that were believed to be related to the extreme fear and stress related to frequent defibrillations delivered by her device. As a final resort, the department of electrophysiology requested evaluation for Video assisted thoracoscopic (VATS) sympathectomy for cardiac denervation.
After the patient is anesthetized and intubated with a double lumen endotracheal tube, a single anterior thoracic 10 mm port incision is made in the 5th intercostal space of the left chest without rib spreading. A 10mm port is inserted, for camera access to the interior of the chest. The left lung is deflated for easy identification and access to the sympathetic nerves at the T2 – T4 level on the chest wall. After successful identification, the nerves were cauterised. The lung was reinflated, and surgical instruments removed. Chest incision was closed with several layers of suture. The patient was awakened, extubated and transferred to the PACU.
In addition to the standard intra-operative hemodynamic and telemetry monitoring, an electrophysiology cardiologist was present during the case to monitor and treat the patient, if necessary.
This slideshow requires JavaScript.
Following surgery, the patient was transferred to the post-anesthesesia care unit (recovery room). Following an uneventful recovery, she was discharged home. At follow-up surgical visit, her incision was well-healed and family reported no further discharges from her AICD.
At six months, post surgery, the patient has had no further cardiac events or ventricular arrhythmias reported or recorded by her device.
Discussion
The cardiovascular effects of sympathectomy have been well-known and described in the medical literature since the early 20th century. However, limitations in surgical technique prior to the advent of thoracoscopic surgery as well as the potential side effects of sympathectomy procedures have limited the use and research into this technique for the treatment of cardiac conditions.
In recent years, researchers at the David Geffen School of Medicine at the UCLA Cardiac Arrhythmia Center (Ajijola et. al) have published several papers about their experiences treating patients with persistant ventricular arrhythmias. In their work, which is one of the largest studies to date, the authors report their experiences with both selective left-sided cardiac sympathetic denervation (LCSD) alone or bilateral cardiac sympathetic denervation (BCSD) as a last-ditch treatment for persistent ventricular arrhythmias. Many of their patients have previously undergone multiple ablation therapies and/or evaluation for cardiac transplantation.
On-going research and clinical trials
Their results have been so promising, in fact, that they have now made cardiac denervation a routine procedure at UCLA and have designed an international multi-center trial called PREVENT VT to study this procedure in a larger group of patients. Since the publication of their initial work, Aijiola et al. have continued their study, with over 40 cases under their belt. Dr. Kalyanam Shivkumar, MD, PhD, Director, UCLA Cardiac Arrhythmia Center & EP Programs reports that they will be presenting their surgical outcomes at an upcoming conference, the Heart Rhythm Meeting at Denver in May of 2013 (Vaseghi et al Cervicothoracic Sympathectomy In Patients With Refractory Vt: Intermediate And Long Term Follow Up).
Contact information for Dr. Kalyanam Shivkumar:
Kalyanam Shivkumar MD PhD
Professor of Medicine & Radiology
Director, UCLA Cardiac Arrhythmia Center & EP Programs
For both their work, and the purposes of this post, persistent ventricular arrhythmias were defined as repeated episodes of ventricular tachycardia or ventricular fibrillation despite maximal medical therapy with a beta blocker and amiodarone**. (In a related article, Ajijola et al. further define which patients are the best candidates for successful outcomes with this procedure.) In their work, the researchers at UCLA were able to show increased effectiveness with the use of bilateral sympathetomy versus left-sided only.
However, the use of left-sided versus bilateral sympathectomy is also determined by the type of arrhythmia (monomorphic versus polymorphic) as well as previous patient history and medical treatments such as catheter based ablations or extensive scar tissue formation from previous cardiac injury.
Given the high morbidity, mortality and adverse effects on the quality of life for people with uncontrolled ventricular arrhythmias as well as the relative low risk, and ease of VATS procedures to treat this condition, cardiac sympathetic denervation should remain an important clinical tool in the treatment of this life-threatening condition, particularly when other treatments have failed.
*Patients with this condition are at very high risk of sudden cardiac risk.
**In the addition to implanted or external defibrillatory devices.
Wilde AA, Bhuiyan ZA, Crotti L, Facchini M, De Ferrari GM, Paul T, Ferrandi C, Koolbergen DR, Odero A, Schwartz PJ. (2008). Left cardiac sympathetic denervation for catecholaminergic polymorphic ventricular tachycardia. N Engl J Med. 2008 May 8;358(19):2024-9. doi: 10.1056/NEJMoa0708006. Case report of a 17 year old boy. In this article, the authors also talk about the psychological trauma experienced by these patients due to frequent defibrillation from AICDs similar to the patient in Colombia.
the latest video from Dr. Diego Gonzalez Rivas demonstrating a sleeve lobectomy via single port surgery
On the heels of the recent conference in Hong Kong, one of our favorite surgeons (and presenter at the 1st Asian single port surgery conference), Dr. Diego Gonzalez Rivas has sent another link to one of his more recent cases – Single port lobectomy – Sleeve resection after chemotherapy.
Gonzalez Rivas, D. (2013). Evolving thoracic surgery: from open surgery to single port thoracoscopic surgery and future robotic. Chinese Journal of Cancer Research, 25 (1) 4-6. Editorial pdf download.
Case report with video of SITS (single incision thoracoscopic surgery) repair of diaphragm defect in a case of hepatic hydrothorax resulting from liver cirrhosis with Dr. Chih-Hao Chen, MAckay Memorial Hospital, Taiwan
Case Report: Single incision thoracoscopic repair of diaphragmatic defect in a patient with hepatic hydrothorax
Dr. Chih-Hao Chen, Thoracic Surgeon MAckay Memorial Hospital, Taiwan
Dr. Chen, Thoracic Surgeon
Clinical History:
Patient is an elderly woman who was admitted after a motor-vehicle accident with a traumatic fracture of the humerus and femoral neck. She was brought to our ED immediately and was intubated due to acute respiratory failure.
Subsequent Chest radiograph showed diffuse opacity in right hemithorax and concomitant fracture in left side humerus and femoral neck. Attempt for tapping of the pleural effusion showed clear in nature.
According to previous medical records, she had no relevant history. She was admitted to ICU for further evaluation and management.
Fluid analysis in emergency department showed transudate.
LFTS: Total Bilirubin 2.7 mg/dL AST 116 ALT 68 Albumin 2.3 g/dL Direct Bilirubin H 1.1 mg/dL
Chem panel: BUN 83 mg/dL Creatinine 1.6 mg/dL K 3.2 mEq/LNa 144 mEq/L
Chest radiograph on admission showed a massive right-sided pleural effusion.
Chest radiograph on admission
For symptomatic control, the physician performed intermittent thoracentesis. Because the traumatic site is left aspect of the trunk ( fracture in left side humerus and left side femoral neck ) and right side effusion was very clear.
Hepatic hydrothorax was suspected. Later peritoneal scan confirmed the diagnosis.
Peritoneal scan
The scan showed left side pleural space was sparring from radioisotope. Direct communication between right side pleural cavity and the abdomen. The diagnosis is confirmed with such findings.
CT scans are not diagnostic for this condition, and were not indicated for her other injuries. Therefore, we did not arrange CT scan of the chest / abdomen.
Abdominal ultrasound showed moderate to massive ascites. Along with hepatic encephalopathy, moderate to massive ascites, prolonged PT/PTT, low albumin, higher bilirubin, the extent of cirrhosis is Child’s class C.
Operative Procedure: Single incision thoracoscopic repair of a diaphragmatic defect. Theoretically, with SITS, the wound can be very tiny. However, in our experience (fifteen total cases to date), diaphragm surgery through single port may be a bit difficult because we did not know where the defect is. We have to inspect very carefully and to search for the defect where the fluid came out. In this case, we made one small wound around 2 cm in length at the 6th ICS along the anterior axillary line.
Repair of the diaphragmatic defect was performed using silk suture similar to that used to repair inguinal hernias. Intra-operatively, the defect was 2 -3 mm in diameter.
At the conclusion of the procedure, using the original incision, we placed one Fr.24 chest tube to monitor the drainage and may consider chemical pleurodesis if the drainage persists. The operative procedure was accomplished within 30 minutes.
Post-operative Chest Radiograph
Post-operative condition of the chest film showed near complete resolution of the effusion and lung re-expansion was complete.
Pathology/ Fluid Cytology: fluid analysis and peritoneal scan showed communication between peritoneal space and right side pleural space confirming pre-operative diagnosis. No tissue specimens were taken during this procedure.
Discussion:
Hepatic hydrothorax is the development of a pleural effusion in a patient with liver disease in the absence of cardiopulmonary pathology, making it a diagnosis of exclusion in many cases. It can occur in patients with and without ascites and may be the first presenting symptom in patients with undiagnosed liver disease. Similar to catamenial pneumothorax; hepatic hydrothorax is predominantly a right-sided disease. This is due to an anatomic gutter or diaphragmatic defect that occurs, and allows the passage of material or fluid from the abdominal cavity into the pleural space. This can be seen and identified on peritoneal studies(Peritoneal scan) like the study showed in our case study above. (Similar pathologies can occur in related conditions such as renal failure related hydrothorax due to this defect). Such defect is usually identified in the tendon part of the diaphragm. Peritoneal scan can confirm there is communication between the abdominal cavity and the pleural space. However, the definite location, size and number of defects can not been identified by the scan alone. Thoracoscopic inspection is the only method to search for such defect(s).
Video-assisted thoracoscopic surgery (VATS) has been shown to be a safe and effective method of treating this condition, by allowing surgeons to correct the defect, and thus prevent recurrence (Saito et al. 2012). The cure rate varied greatly in the literature. The key is whether the defect can be repaired. For one to two obvious defects, direct suture repair usually cured the disease. (the cure rate more than 80%) However, for some undetectable defects or defects with fenestration type, the cure rate is very low, ( around 30-50% ). Alternative strategies have to be considered in such condition, such as tissue glue, abrasion pleurodesis, mesh interposition and using sclerosing agents(OK432, bleomycin, Minocin, talc, etc). This is in distinct contrast to the numerous non-surgical drainage procedures such as thoracentesis, which removes accumulated fluid but does not correct the underlying pathology. However, the hallmark of this condition, liver failure predisposes patients to complications such as bleeding, infection and poor wound healing. These risks are one of the primary reasons treatment was often limited to drainage procedures prior to the popularization of lower risk VATS procedures. In the past, patients with Child’s class C liver cirrhosis are basically not proper surgical candidates because of extremely high mortality/morbidity rate. In recent experience of single-port approach, some patients with Child B and C are still safe with minimal postoperative complications. The advance of these minimally invasive technologies such as uni-port thoracoscopy permits fewer and more limited incisions which is believed to further reduce these risks while providing patients with definitive treatment options. More case studies such as this one, along with larger studies are needed to demonstrate the benefits of this technique for hepatic hydrothorax.
References
Doraiswamy V, Riar S, Shrestha P, Pi J, Alsumrain M, Bennet-Venner A, Kam J, Klukowicz A, Miller R. (2011). Hepatic hydrothorax without any evidence of ascites. ScientificWorldJournal. 2011 Mar 7;11:587-91. doi: 10.1100/tsw.2011.68 Case study.
Lee WJ, Kim HJ, Park JH, Park DI, Cho YK, Sohn CI, Jeon WK, Kim BI. (2011). Chemical pleurodesis for the management of refractory hepatic hydrothorax in patients with decompensated liver cirrhosis. Korean J Hepatol. 2011 Dec;17(4):292-8. doi: 0.3350/kjhep.2011.17.4.292. Eleven patient Korean study looking at the effectiveness of pleurodesis in patients with hepatic hydrothorax. While the procedure was successful in 8 patients, the authors noted a high rate of procedural-associated complications. (Notably, the researchers used several different agents for chemical pleurodesis.)
Sawant P, Vashishtha C, Nasa M. (2011). Management of cardiopulmonary complications of cirrhosis. Int J Hepatol. 2011;2011:280569. doi: 10.4061/2011/280569. Epub 2011 Jul 19. Article discussing complications of cirrhosis including hydrothorax.
Interested in learning more about single port thoracoscopy, or talking to the inventors of this technique? This March – head to the 1st Asian single port surgery conference in Hong Kong.
It doesn’t look like Cirugia de Torax will be in attendance for this conference, but it’s another opportunity for practicing thoracic surgeons and thoracic surgery fellows to learn more about single port thoracoscopic surgery.
This March (7th – 8th), the Chinese University of Hong Kong, along with the Minimally Invasive Thoracic Surgery Unit (Coruna, Spain), and Duke University are presenting the 1st Asian Single Port Symposium and Live Surgery conference in Hong Kong.
This is your chance to meet the experts – and the inventors of this technique (such as Dr. Diego Gonzalez – Rivas, one of the new masters frequently featured here at Cirugia de Torax.)
a day in the operating room with one of Colombia’s New Masters of Thoracic Surgery
Cali, Colombia
Dr. Mauricio Velasquez is probably one of the most famous thoracic surgeons that you’ve never heard of. His thoracic surgery program at the internationally ranked Fundacion Valle del Lili in Cali, Colombia is one of just a handful of programs in the world to offer single port thoracic surgery. Dr. Velasquez has also single-handedly created a surgical registry for thoracic surgeons all over Colombia and recently gave a presentation on the registry at a national conference. This registry allows surgeons to track their surgical data and outcomes, in order to create specifically targeted programs for continued innovation and improvement in surgery (similar to the STS database for American surgeons).
Dr. Mauricio Velasquez after another successful case
Dr. Velasquez is also part of a team at Fundacion Valle del Lili which aims to add lung transplant to the repertoire of services available to the citizens of Cali and surrounding communities.
He is friendly, and enthusiastic about his work but humble and apparently unaware of his growing reputation as one of Colombia’s finest surgeons.
Education and training
After completing medical school at Universidad Pontificia Bolivariana in Medellin in 1997, he completed his general surgery residency at the Universidad del Valle in 2006, followed by his thoracic surgery fellowship at El Bosque in Bogotá.
The Colombia native has also trained with thoracic surgery greats such as Dr. Thomas D’Amico at Duke University in Durham, North Carolina, and single port surgery pioneer, Dr. Diego Gonzalez Rivas in Coruna, Spain. He is also planning to receive additional training in lung transplantation at the Cleveland Clinic, in Cleveland, Ohio this summer.
Single port surgery
Presently, Dr. Velasquez is just one of a very small handful of surgeons performing single port surgery. This surgery is an adaptation of a type of minimally invasive surgery called video-assisted thoracoscopy. This technique allows Dr. Velasquez to perform complex thoracic surgery techniques such as lobectomies and lung resections for lung cancer through a small 2 – 3 cm incision. Previously, surgeons performed these operations using either three small incisions or one large (10 to 20cm) incision called a thoracotomy.
By using a tiny single incision, much of the trauma, pain and lengthy hospitalization of a major lung surgery are avoided. Patients are able to recovery and return to their lives much sooner. The small incision size, and lack of rib spreading means less pain, less dependence on narcotics and a reduced incidence of post-operative pneumonia and other complications caused by prolonged immobilization and poor inspiratory effort.
However, this procedure is not just limited to the treatment of lung cancer, but can also be used to treat lung infections such as empyema, and large mediastinal masses or tumors like thymomas and thyroid cancers.
Dr. Velasquez in the operating room with Lina Caicedo Quintero (nurse)
Team approach
Part of his success in due in no small part to Dr. Velasquez’s surgical skill, another important asset to his surgical practice is his wife, Dr. Indira Cujiño, an anesthesiologist specializing in thoracic anesthesia. She trained for an additional year in Spain, in order to be able to provide specialized anesthesia for her husband’s patients, including in special circumstances, conscious sedation. This allows her husband to operate on critically ill patients who cannot tolerate general anesthesia. While Dr. Cujiño does not perform anesthesia for all of Dr. Velasquez’s cases, she is always available for the more complex cases or more critically ill patients.
In the operating room with Dr. Velasquez
I spent the day in the operating room with Dr. Velasquez for several cases and was immediate struck by the ease and adeptness of the single port approach. (While I’ve written quite a bit about the literature and surgeons using this technique, prior to this, I’ve had only limited exposure to the technique intra-operatively.) Visibility and maneuverability of surgical instruments was vastly superior to multi-port approaches. The technique also had the advantage that it added no time, or complexity to the procedure (unlike robotic surgery).
Dr. Velasquez performing single port thoracoscopy
Cases proceeded rapidly; with no complications.
close up view
Note to readers – some of the content, and information obtained during interviews, conversations etc. with Dr. Velasquez may be used on additional websites aimed at Colombia-based readers.
an Interview with Dr. Diego Gonzalez Rivas – and coverage of ‘Videotoracoscopia y cirugia robotica en torax: Avances y perspectivas’ in Santiago, Chile
Santiago, Chile
I was a little intimidated to actually interview Dr. Diego Gonzalez Rivas after reading his articles and pestering him with emails for the last few years. But he was just as nice and patient with my questions as he’s always been.
Dr. Santolaya, Dr. Sales dos Santos, Dr.Berrios and Dr. Diego Gonzalez Rivas
Since publishing the last few articles on his single port technique, Dr. Gonzalez has been in high demand from thoracic surgeons wanting to learn more, and to train in single port techniques. In addition to traveling the world to teach – he continues to offer training at the Minimally Invasive Thoracic Surgery Unit at the Complexo Hospitalario Universitario de A Coruna, in Coruna, Spain.
Dr. Gonzalez reports that single port thoracoscopy doesn’t just provide patients with the least invasive surgery possible, but that single port thoracoscopy is superior to traditional VATS in the vast majority of cases. Single port thoracoscopy is defined by the creation of one 2cm to 4cm incision – with no rib spreading and utilization of video-assisted thoracoscopy.
“Forward Motion”
He states that using a single port approach gives much better visibility than traditional VATS. This visibility is equal to that of open surgery – versus the 3 or 4 port approach, which is constrained by the 30 degree movement / rotation of the thoracoscope. This visibility concept; called ‘Forward Motion,’ along with the ease of using instrumentation through the same port makes single port surgery amendable to most thoracic surgery procedures.
Learning curve? What learning curve?
He reports that members of the “Playstation Generation” as he terms the newest young surgeons, adapt more readily to the use of both traditional and single port thoracoscopy. In fact, he reports that the residents (in his program) are able to learn and use this approach with minimal assistance.
With the exception of lung transplantation (requiring the traditional clamshell incision), Dr. Gonzalez reports that he is able to successfully perform a wide range of surgeries from wedge resections and lobectomies to more complicated procedures such as pneumonectomies and sleeve resections.
In today’s lecture he debunks some of the myths regarding the ‘classic contraindications’ to video-assisted thoracoscopy (VATS) such as broncheoplasty, the presence of dense adhesions or the need for complete lymph node dissection. While he reports that dense adhesions may make the procedure more painstaking and difficult – it is still possible.
LymphNode Dissection
In cases of lymph node dissection – he reports that lymphadenectomy is actually superior by single port and other VATS methods, with the average surgeon actually harvesting more nodes, more easily.
While he initially believed that right upper lobe resections would be impossible with this method – his recent experiences (included in an upcoming paper on 102 cases) show that any anatomic complexities are readily overcome by an experienced VATS surgeon. Not only that, but he has been able to successfully remove very large (8cm or greater) lung tumors using this method – by slightly enlarging the port at the time of specimen removal. He has also successfully removed Pancoast tumors and performed chest wall resections with this procedure, as well as single port thoracoscopy after previous VATS or previous thoracotomy including completion pnuemonectomies and completion sleeve lobectomies.
One of the biggest obstacles for surgeons implementing the single port method is the dreaded complication of catastrophic bleeding. This often causes inexperienced single port surgeons to hasten to convert to open surgery without attempting to control the bleeding. Dr. Gonzalez presented several cases today to demonstrate the difference between controlled bleeding that can be managed with the speedy application of surgical staples, clips or sutures versus heavy uncontrolled bleeding, which requires quick recognition and prompt conversion to open thoracotomy.
He reports that in the over 500 cases he has performed by VATS (3 port, dual port and single port), conversion to open thoracotomy remains a very rare occurence. (He presented data on his outcomes today.)
In his own practice, he reports that prior to 2007 the majority of cases were by traditional thoracotomy. He began using 3 port VATS more heavily in 2007 – 2009. After training with Dr. D’Amico at Duke University in Durham, NC – he moved to dual port thoracoscopy in 2009. Since 2010, his practice is almost exclusively single port thoracoscopy.
The future of single port thoracoscopy
Dr. Gonzalez believes the future of single port thoracoscopy will be a hybridization of current robotic thoracic surgery (which now uses three and four port techniques) to using less invasive, smaller robotic arms that will allow surgeons to enjoy the micro-precision of robotic technology through a single port.
Not just a ‘single port surgeon’
While he is famous internationally for his innovations in the field of minimally invasive surgery, he is also a transplant surgeon. In fact, along with his partners, he performed an average of 35 – 40 lung transplants a year.* This makes the transplant program in Coruna the second largest in Spain, despite the relatively small size of Coruna compared to other cities such as Barcelona or Madrid.
For patients who are interested in Dr. Gonzalez-Rivas and his program, please contact him at Info@videocirugiatoracica.com
I published an article based on this interview over at Examiner.com
5 / Video-assisted thoracic surgery lobectomy: 3-year initial experience with 200 cases. Gonzalez D, De la Torre M, Paradela M, Fernandez R, Delgado M, Garcia J,Fieira E, Mendez L. Eur J Cardiothorac Surg. 2011 40(1):e21-8.
6 / Single-port Video-Assisted Thoracoscopic Anatomical Resection: Initial Experience. Diego Gonzalez , Ricardo Fernandez, Mercedes De La Torre, Maria Delgado, Marina Paradela, Lucia Mendez. Innovations.Vol 6.Number 3. May/jun 2011. Page 165.
Books/ Book Chapters
1 / Thoracoscopic lobectomy through a single incision. Diego Gonzalez-Rivas, Ricardo Fernandez, Mercedes de la Torre, and Antonio E. Martin-Ucar. Multimedia Manual of Cardio-Thoracic Surgery. MMCTS (2012) Vol. 2012 doi:10.1093/mmcts/mms007. Includes multiple videos demonstrating single port techniques.
2 / Tumores del diafragma. M. de la Torre Bravos, D. González Rivas, R. Fernández Prado, JM Borro Maté. Tratado de Cirugía Torácica. Editores L. Fernandez Fau, J. Freixinet Gilart. SEPAR Editores médicos SA. Madrid 2010. Vol 2, Sec VIII, Capitulo 87: 1269-78.
3 / Trasplante Pulmonar. C. Damas, M. De la Torre, W. Hespanhol, J.M. Borro. Atlas de Pneumología. Editores A. Segorbe Luís y R. Sotto-Mayor 2010. Vol 2, Capítulo 54 651-8.
4 / Doble utilidad hemostática y sellante de fuga aérea de tachosil en un caso de cirugía compleja por bronquiectasias. M. De la Torre, J.M. Borro, D. González, R. Fernández, M. Delgado, M. Paradela. Anuario 2009. Casos clínicos en cirugía. Accesit en la 3ª edición de los Premios Nycomed 2008.
5 / Cirugía Torácica videoasistida avanzada. D. González Rivas. Videomed 2008. Certamen internacional de cine médico y científico.
6 / Traumatismo Torácico. M. de la Torre, M. Córdoba. En « Manual de Urgencias en Neumología». Editado por Luis M Domínguez Juncal, 1999 165-78.
7 / Neumotórax. M. Córdoba, M. de la Torre. En « Manual de Urgencias en Neumología». Editado por Luis M Domínguez Juncal, 1999 139-56.
8 / Cirugía del enfisema. P. Gámez, J.J. Rivas, M . de la Torre. En « Neumología Práctica al Día». Boehringer Ingelheim 1998 77-102.
9 / Neumotórax. J.J. Rivas, J. Torres, M. de la Torre, E. Toubes. En « Manual de Neumología y Cirugía Torácica». Editores Médicos S.A. 1998 1721-37.
Dr. Chen discusses single port thoracoscopy – and specimen size.
Single port thoracoscopy for wedge resection – does size matter? Dr. Chih-Hao Chen, Thoracic Surgeon, Mackay Memorial Hospital, Taiwan Correspondence: musclenet2003@yahoo.com.tw
Case presentation and discussion
A 77 y/o woman was found to have a neoplasm in RML during routine health exam. (Full case presentation here.)
The incision was 2.5 cm. The specimen was removed successfully; patient experienced no complications and was discharged from the hospital without incident. However, when discussing this case with surgeon colleagues a specific question arose.
preparing to remove the specimen through the port
Does size matter? How big is too big to remove through a port incision?
An important issue is the theoretically smallest (and effective) incision size. The issue is very challenging for most surgeons. In the past, other surgeons have questioned me :
“The specimen to be removed is more than 12-15 cm. How can you remove the specimen from a 3.5 cm incision?”
BUT, the fact is “the smallest size depends mostly on the solid part of the neoplasm “.
The lung is soft in nature. In my experience, a 3.5 cm port is usually enough for any lobe. The only problem is that if the solid part is huge, pull-out of the specimen may be difficult.
Therefore, the solid part size is probably the smallest incision size we have to make, usually in the last step when dissection completed , if needed.
successful removal of lung specimen thru small port
Port with chest tube in place
Using endo-bags to avoid larger incisions
There is an exception. I have never do this but I think it may be possible. We usually avoid opening the tumor (or cutting tumor tissue into half ) within the pleural space in order to prevent metastasis from spillage of cancerous tissue.
What if we can protect the tumor from metastasis while we cut it into smaller pieces? For example, into much smaller portions that will easily pass through the small port incisions?
My idea is to use double-layer or even triple layers of endo-bag to contain the specimen. If it is huge, with perfect protection, we cut it into smaller parts within the bag. Then the huge specimen can be removed through a very tiny incision. This is possible.
We still have to avoid “fragmentations” since this might interfere or confuse the pathologist for accurate cancer staging. Therefore, in theory, we can cut it into smaller parts but not into fragments. However this idea is worthy of consideration, and I welcome debate from my fellow surgeons and medical colleagues.
Dr. Chih-Hao Chen at Mackay Memorial Hospital in Taiwan talks about his experiences with single port/ single incision thoracic surgery (SITS) as well as the “Chen esophagectomy”; a new single port approach to esophagectomies.
Single-port thoracoscopic surgery (SITS) as a first-line approach
With the advent of minimally invasive surgical techniques such as VATS, surgeons now have the ability to perform multiple surgical procedures such as lobectomy, decortication and even esophagectomy through 1 – 2 cm port incisions instead of traditional open surgery. However, as mentioned during an interview with Dr. Mark Dylewski, few American* surgeons have fully embraced this technology. Even fewer surgeons internationally have embraced the emerging single port techniques that have developed from VATS. One of these surgeons is Dr. Chih-Hao Chen at Mackay Memorial Hospital in Taiwan. We previously discussed one of his studies here at Cirugia de Torax, so it was with great delight when we had an opportunity to discuss his continuing research and development in this area in a series of emails.
Dr. Chen is currently in the forefront of the movement to make SITS a first-line approach for majority of thoracic surgery procedures that can currently be approached with traditional VATS. The biggest risk to this “less is more” approach to port placement is needing to add additional ports during the case (thus converting to traditional VATS 3-4 port approach).
As Dr. Chen explains, “In contrast to creating 3 small wounds, I always try single-port first. If it is technically unavoidable, I would make the second port incision. If it is still difficult, a third port incision would be made. The conversion rate (to 2-port or three port methods not open) is very low in most conditions.
“I believe the role of SITS as a first-line endoscopic approach is possible in nearly all patients. So far, I have performed roughly, SITS in more than 150 patients with various thoracic diseases, including esophagectomy in 5 cases using 2.5 cm single incision”.
However, the contraindications for the SITS approach are mainly those with “unstable hemodynamics in trauma”, “highly complicated cancer resection(such as sleeve lobectomy, etc)” and “thick and dense peel in chronic empyema”.
Dr. Chen was kind of the provide this clip of him performing single port thoracoscopy.
Over 150 cases, so far.
“According to my experience, patients with spontaneous pneumothorax and acute stage empyema as well as solitary pulmonary nodules are the best candidates for such procedure. The time required for the same operation is much shorter in single-port approach. For simple spontaneous pneumothorax, the time may be as short as 20-25 minutes. ( from skin incision to suture )”.
As I mentioned in my report (see publications linked below), the conversion rate of such condition is pretty low and worthy to try. In my experience, SITS w/o trocar greatly decrease incisional pain and have pleasant cosmetic results, as the wound can be extremely small”.
A recent case: Wedge resection by SITS
Procedure: single-port approach for a case of lung cancer in a 77 year-old woman.
Multiple wedge resections, pleural biopsy and LN smapling were performed.
single incision (now with chest tube) and specimen removed (photo courtesy of Dr. Chen)
The wound was 1.5 cm in length and the specimen is 7cm X 4cm ( solid part :2.5 cm ). The specimen was removed within an endo-bag. (From previous experience, I knew that a specimen of this size can be safely removed through a tiny incision w/o destruction of the specimen.
Her chest tube was removed within 24 hrs and patient reports minimal discomfort. ( I injected Marcaine in ICS to prevent neuralgia in all cases.)
Sometimes innovation is hard
As we’ve seen frequently in the history of medicine / surgery, early innovators and adopters of new technology are often face significant resistance from their colleagues despite utilizing ‘best-evidence’ to support their ideas. People, many people, including surgeons – don’t like change and are sometimes hesitant to learn and practice techniques that develop in the years following fellowship.
One of the reasons Dr. Chen contacted Cirugia de Torax is to share his experiences and this technique with other interested thoracic surgeons. ‘Unfortunately, only a small portion of thoracic surgeons would like to try such procedure in Taiwan. Actually, most of them considered the procedure not valuable. Therefore, I would like to publish more experiences in the journals, which is one way to tell them “to try”.
Wait.. Did you say single-port thoracoscopy for esophagectomy?
“Esophagectomy in my team was performed by single-port thoracoscopic approach (in the chest). However, the abdominal portion was performed with four-port or 5-port laparoscopic approach, because the abdominal part was done by another doctor who is not familiar with single-incision laparoscopy (SILS). However, I have to admit that esophagectomy through single-port approach is much more difficult than other procedures. The main reason for this is that the esophagus is located in posterior mediastinum.”
While I usually utilize a more anterior ICS as my port incision for other single-incision procedures because the anterior ICS is very easy, with low conversion ( to 2- or 3-port ) rate. However, the same port is not appropriate for esophagectomy because of poor visualization.
New Approach, the “Chen esophagectomy” but ergonomic considerations
“For the reason, I tried a more lateral port incision (usually 5 ICS along the mid-axillary line. ) This is a BIG problem for me due to ergonomic issues. Manipulation of endoscopic instruments and the endoscope through the port is uncomfortable. At times, I have to rest for a while in order to alleviate soreness in my arm”.
“The time-determining step is to loop the esophagus. Proximal and distal dissection as well as lymph node dissection would be done with a harmonic scalpel. (We resected the esophagus, the anastomosis is in the neck ). For uncomplicated case, the procedure in the chest takes aroud 1-2.5 hours”.
*American research data suggests that VATS is used for less than 30% of all thoracic surgery procedures. However, anecdotal evidence suggests that internationally, VATS is utilized with much higher frequency outside of the United States.
Articles about single-incision thoracoscopic surgery (SITS) by Dr. Chih-Hao Chen
Robotic (thoracic) surgery comes to Clinica de Marly in Bogota, Colombia
A year and a half ago, I interviewed and spent some time with Dr. Ricardo Buitrago at the National Cancer Institute, and Clinica de Marly while doing research for a book about thoracic surgeons. At that time, Dr. Buitrago stated he was interested in starting a robotic surgery program – and was planning to study robot-assisted thoracic surgery with Dr. Mark Dylewski.
Dr. Ricardo Buitrago in the operating room, April 2011
Fast forward 1 year – when I received a quick little email from Dr. Buitrago telling me about his first robotic surgery at the Clinica de Marly. At that point, I sent Dr. Buitrago an email asking if I could come to Colombia and see his robotic surgery program to learn more about it. We had several phone conversations about it and I also outlined a research proposal to gather data on thoracic surgery patients and outcomes at high altitude, to which he enthusiastically offered to assist with. Thus began my current endeavor, in Bogota, studying with Dr. Buitrago.
Now – after completing a proctoring period with Dr. Dylewski, Dr. Buitrago has more than a dozen independent robotic surgeries under his belt. He has successfully used the robot for lobectomies, mediastinal mass resections and several other surgeries.
As part of my studies with Dr. Buitrago – I’ve made a video for other people who may be interested in robotic surgery with the DaVinci robot and what it entails.
One of the world’s experts on sympathectomy and the treatment of hyperhidrosis reviews the evidence at the XVI Congreso Boliviano Sociedad de Cirugia Cardiaca, Toracica y Vascular 2012.
While there was no opportunity to speak with Dr. Jose Ribas de Milanez de Campos at length, Cirugia de Torax did have a chance to talk briefly with the world-renown Brazilian thoracic surgeon about his presentation on VATS sympathetectomy for the treatment of hyperhidrosis. He is one of the foremost experts on hyperhidrosis and the treatment of this condition. (He, along with other thoracic surgery legends, Cefalio and McKenna helped draft the STS statement of the topic.)
Dr. Jose Ribas de Milanez de Campos
Dr. Ribas reviewed the current literature as well as the most recent ATS Expert Consensus, and changes in international nomenclature for the ongoing research in the treatment of hyperhidrosis.
State of the evidence
At the 2009 American Thoracic Society expert consensus for surgical treatment of hyperhidrosis – a meta-analysis of the existing data was performed. Of the 1097 different papers, there were just 102 detailing clinical trials. Of these, only 12 studies met the criteria as randomized trials, and these studies were conducted by just three different groups of surgeons. Findings were based on this small pool of data.
Changes in nomenclature
Following the review of this data, several changes in surgical nomenclature were suggested to increase the clarity of data reporting among surgeons. One of the main points of confusion is the use of the ganglia level to report and describe procedures. This is problematic since multiple studies, including cadaveric studies, have shown that there are multiple anatomic variations in ganglia level. Also obese body habitus may obscure landmarks/ levels of ganglia in the fat tissue. Thus, the ATS now suggests that surgeons use “Rib Level” when reporting sympathectomy procedures. This is believed to allow greater precision and accuracy in data reporting.
Surgeons are also encouraged to classify surgical procedures as either sympathetomy, sympathiocomy or ramicotomy – mentioning the mechanism of sympathetic interruption; clipped versus cut, cauterised or otherwise removed. There is no clearly superior method but surgeons need to be sure that there is enough separation between the ends of the sympathetic chains. Dr. de Campos prefers dual port incisions over single port access for better visibility, and considers the harmonic scalpel much more precise.
The third major recommendation for surgeons performing sympathetectomies – is the recommended use of quality of life questionnaires for periodic follow-up with patients.
Treating hyperhidrosis
Level of sympathetic interruption should be related to patient’s primary symptomatology.
R2, R3 for patients with facial symptoms such as facial flushing.
R3 & R4 for patients with palmar symptoms.
R4 & R5 for patients with palmar and (severe) axillary sweating.
This is important because patients report greater satisfaction, less regrets and less side effects with the lower level blockages (R4 versus R2). Due to the inexactness of reports and poor follow-up, it is hard to know the incidence of compensatory hyperhidrosis (or compensatory sweating of lower extremities). Literature has reported the incidence at 3% – 98% of patients, making it difficult to quantify.
Patients who have sympathetic interruption of both R2 & R3 increases the risks of compensatory hyperhidrosis and Horner’s syndrome. This compensatory sweating is also more severe in warmer climates.
Best Candidates for the procedure
The best candidates for the procedure are patients who developed symptoms at an early age. Palmar symptoms often begin in young children (including toddlers). Axillary symptoms usually start during adolescence, with craniofacial symptoms beginning in young adulthood.
Surgery is most effective in younger patients (under the age of 25). Patients also need to be of normal weight for the best results with a BMI of 25 or less*. This is important because the greater the weight (or body mass index), the higher the incidence of compensatory sweating – which will prevent effective surgical treatment.
Common complications
The most common complications are compensatory sweating, and Horner’s syndrome. This occurs more frequently with higher level surgeries.
When to have surgery
Patients should consider surgery only after exhausting other treatments – as the expert consensus states sympathectomy should be considered a procedure of “last resort.”
However, oxybutynin treatment has shown promise for the treatment of hyperhidrosis. After 45 to 90 days of oxybutynin treatment, 80% of patients will respond favorably with noticeable improvement in symptoms. Surgery should be reserved for refractory cases.
*BMI of 28 or less in the United States, according to national guidelines.
References
Includes a limited list of publications by Dr. Rivas de Milanez de Campos on this topic.
M.A. Callejas, R. Grimalt, E. Cladellas (2010). Hyperhidrosis update.Dermo-Sifiliográficas (English Edition), Volume 101, Issue 2, March–April 2010, Pages 110-118.
Cameron AE, Connery C, De Campos JR, Hashmonai M, Licht PB, Schick CH, Bischof G; International Society of Symapathetic Surgery. Percutaneous chemical dorsal -sympathectomy for hyperhidrosis. Minim Invasive Neurosurg. 2011 Oct;54(5-6):290. Epub 2012 Jan 25 [letter].
De Campos JR, Hashmonai M, Licht PB, Schick CH, Bischof G, Cameron AE, Connery CP. (2012). Treatment options for primary hyperhidrosis. Am J Clin Dermatol. 2012 Apr 1;13(2):139. [comment].
de Campos JR, Kauffman P, Werebe Ede C, Andrade Filho LO, Kusniek S, Wolosker N, Jatene FB. (2003). Quality of life, before and after thoracic sympathectomy: report on 378 operated patients. Ann Thorac Surg. 2003 Sep;76(3):886-91. [full-text not available.]
Wolosker N, Yazbek G, Ishy A, de Campos JR, Kauffman P, Puech-Leão P. (2008). Is sympathectomy at T4 level better than at T3 level for treating palmar hyperhidrosis? J Laparoendosc Adv Surg Tech A. 2008 Feb;18(1):102-6. [full-text not available.]
For additional information on this topic:
Nauman, M., Davidson, J. R. T. & Glaser, D. (2002). Hyperhidrosis: Current Understanding, Current Therapy. Medscape. [Registration required for Medscape]. Click article title for pdf version. While this article is dated back to 2002, it gives a good overview of hyperhidrosis for people who are unfamiliar with this condition.
A newly published study comparing dual port thoracoscopy with mini-thoracotomy for the treatment of recurrent spontaneous pneumothorax
Here at cirugia de torax, we take a keen interest in the development of increasingly minimally invasive technologies from dual (and single-port) thoracoscopy for a variety of conditions to RATS (robot- assisted thoracic surgery). It is our belief that by embracing these emerging technologies, we help to advance the thoracic surgery specialty.
This spring, we have had the pleasure of publishing case reports on dual port thoracoscopy for decortication of parapneumonic effusions and empyema and catching up with one of the leaders in single incision thoracic surgery, Dr. Diego Gonzalez Rivas.
This month, another entry, “A modified two-port thoracoscopic technique versus axillary minithoracotomy for the treatment of recurrent spontaneous pneumothorax: a prospective randomized study,” by Dr. Christophoros N. Foroulis at the Aristotle Medical School in Thessaloniki, Greece was published in SurgicalEndoscopy. As noted in a previous post, there have been few (if any) published papers on dual port thoracoscopy, and no comparison studies of these two techniques.
This study, which was conducted during 2006 to 2009 followed 66 patients who were randomly assigned to receive either mini-thoracotomy or dual-port VATS for surgical pleurodesis/ bullectomy / blebectomy.
In this study, despite random assignment, each group of 33 patients were well matched in all characteristics such as age, operative side and BMI. After surgical treatment, patients were followed for a median of 30 months (range 3 – 53 months) for development of late complications or recurrent pneumothorax.
Each treatment group – VATS versus open surgical was overseen by one surgeon with Dr. Foroulis performing all of the dual port surgeries, and Dr. Papakonstantinou performing all of the open procedures. Outcomes were independently reviewed / evaluated by the remaining authors.
Study Findings
– No conversions to open thoracotomy from the VATS group.
– Similar rate of recurrence between open (2.7%) and VATS (3%) group (but timing of recurrence differed.) Both recurrent pneumothoraces in the VATS group occurred early post-operatively (POD#5) compared to the open surgical group – 13 months post-op.
– Rate of complications the same between groups but the type of complications differed. 2 patients in each group required reoperation:
VATS – reoperation for prolonged airleak
Minithoracotomy group – hematomas/ evacuation of clots
Length of stay (LOS) and post-operative pain
Surprisingly, length of stay and post-operative pain – two of the outcomes that are usually cited in favor of minimally invasive procedures – were not significantly different between the groups.
Differences
Patient satisfaction
However, patient satisfaction was significantly higher in the dual port group. This was related to an earlier return to normal activities, and earlier full mobilization of the affected arm.
Longer procedures
VATS procedures were longer than open procedures – by a mean of 21 minutes (87.1 minutes for VATS versus 66.7 minutes for minithoracotomy) with associated increases in uni-lung ventilation time.
Discussion/ Conclusions
While previous studies had reported a recurrence rate that was significantly higher in the VATS group – that was not seen here. The ability to detect blebs/ bullae (and thus treat) with VATS remains limited in comparison to a mini-thoracotomy, but does not appear to change outcomes after a successful pleurodesis procedure. Dual port thoracoscopy does take more time but both procedures appear equally effective.
Reference:
Foroulis, C. N., Anastasiadis, K., Charokopos, N., Antonitisis, P., Halvatzoulis, H. V., Karapanagiotidis, G. T., Grosomanidis, V. & Papakonstantinou, C. (2012). A modified two-port thoracoscopic technique versus axillary minithoracotomy for the treatment of recurrent spontaneous pneumothorax: a prospective randomized study. Surg Endosc 2012 May 12. Includes color photographs of procedures.
This case study was prepared with assistance from Dr. Carlos Ochoa. Since we have been discussing the relevance of case reports and providing tips on case report writing for new academic writers – we have written the following case report in the style advocated by McCarthy & Reilley (2000) using their case report worksheet to demonstrate the ease of doing so in this style.
Since the previous presentation of dual-port thoracoscopy for decortication was missing essential materials, we are presenting a second case report.
Authors: K. Eckland, ACNP-BC, MSN, RN & Carlos Ochoa, MD
Case Report: Dual port thoracoscopy for decortication of a parapneumonic effusion
Abstract: The use of increasingly minimally invasive techniques for the treatment of thoracic disease is becoming more widespread. Dual and even single port thoracoscopy is becoming more frequent in the treatment of parapneumonic effusions and empyema.
Clinical question/problem: the effectiveness and utility of dual port thoracoscopy for parapneumonic effusions.
Analysis of literature review: Despite the increasing frequency of dual and single port thoracoscopic techniques, there remains a dearth of literature or case reports on this topic. Pubmed and related searches reveal only a scattering of reports.
Summary: As the case report suggests, dual port thoracoscopy is a feasible and reasonable option for the treatment of parapneumonic effusion.
Case history: 50-year-old patient with a three-week history of pneumonia, with complaints of right-sided chest pain, cough and increased phlegm production. Additional past medical history is significant for poorly controlled diabetes, hypertension, and obesity with central adiposity. Medications included glyburide and lisinopril.
After being seen and evaluated by an internal medicine physician, the patient was started on oral antibiotics. After three weeks, when his symptoms failed to improve, he was referred by internal medicine to thoracic surgery for out-patient evaluation.
On exam: middle-aged obese diabetic gentleman in no immediate distress, resting comfortable in the exam room. Face appeared moderately flushed, but skin cool and dry to the touch, no evidence of fever.
On auscultation, he had diminished breath sounds over the right lower lobe with egophony over the same area. The remainder of the exam was essentially normal.
Lab studies showed a mildly elevated WBC of 11.6, decreased Hgb of 10.4 / HCT 32.5. Hemoglobin A1c 10.6, Fasting glucose 228, HDL mildly low at 40.
EKG showed slight axis deviation, with slightly prolonged QRS complex (.16) with no evidence of loss of R, St elevation or other abnormalities. He was cleared by internal medicine for surgery.
After risks, benefits and alternatives to VATS decortication were explained to the patient – the patient consented to proceed with surgical decortication. After scheduling surgery, the patient was seen by anesthesia in preparation for the procedure.
Surgical procedure: Dual-port thoracoscopy with decortication of parapneumonic effusion.
Dual port thoracoscopy
After being prepped and drapped in sterile fashion and confirmation of dual lumen endotracheal tube placement, a small 2 cm incision was made for insertion of a 10mm port. Following entry into the chest with the thoracoscope, the right lung was deflated for optimal inspection and decortication of loculations. After completing the majority of the procedure, a second access port was created for better visualization and to ensure that a thorough decortication was completed. The lung and pleural were separated from the chest wall, and diaphragm, and demonstrated good re-expansion with lung re-inflation prior to completion of the procedure.
chest tubes at conclusion of case
At the conclusion of the procedure, two 28 french chest tubes were placed in the existing incisions. These were sutured into place, and connected to a pleurovac drainage system before applying a sterile gauze dressing. The patient remained hemodynamically stable throughout the case, with no episodes of hypoxia or desaturation. Following surgery, the patient was transferred to the PACU in stable condition.
Post-operative course was uncomplicated. Chest tubes were water-sealed on POD#3 and chest tubes were removed POD#4, with the patient being subsequently discharged after chest x-ray.
close up view of dual port thoracoscopy
Literature Review
A literature review was performed on PubMed using “dual port thoracoscopy”, “dual port VATS”, “2 port” as well as minimally invasive thoracoscopic surgery “
Results of search: A limited number of case studies (3) described thoracoscopic surgery with a single port. There was one case found describing cases conducted with two ports, and the majority of reports involved three or more access ports.
Discussion/ Conclusion
While convention medical wisdom dictates a trial and error treatment approach with initial trial of antibiotic therapy followed by chest tube placement (Light, 1995), surgeons have long argued that this delay in definitive treatment places the patient at increased risk of significant morbidity and mortality (Richardson, 1891). Multiple recent reviews of the literature and research comparisons continue to demonstrate optimal outcomes with surgery based approaches versus antibiotics alone, TPA and tube thoracostomy. The ability to perform these procedures in the least invasive fashion (VATS versus thoracotomy approaches) defies the arguments against surgical intervention as advanced by interventionalists (radiologists and pulmonologists.) Successful decortication with the use of dual port thoracoscopy is another example of how technology is advancing to better serve the patient and provide optimal outcomes, and offers a minimally invasive option when single port surgery may not be feasible.
During the case above, visibility and access to the thoracic cavity was excellent. However, in cases requiring additional access, reversion to the standard VATS configuration can be done easily enough with significant delays or additional risks to the patient.
References/ Resources
Foroulis CN, Anastasiadis K, Charokopos N, Antonitsis P, Halvatzoulis HV, Karapanagiotidis GT, Grosomanidis V, Papakonstantinou C. (2012). A modified two-port thoracoscopic technique versus axillary minithoracotomy for the treatment of recurrent spontaneous pneumothorax: a prospective randomized study. Surg Endosc. 2012 Mar;26(3):607-14. [free full text not available.]
Gonzalez – Rivas, D., Fernandez, R., De la Torre, M., & Martin – Ucar, A. E. (2012). Thoracoscopic lobectomy through a single incision.Multimedia manual cardio-thoracic surgery, Volume 2012. This is an excellent article which gives a detailed description, and overview of the techniques used in single incision surgery. Contains illustrations, full color photos and videos of the procedure.
Gonzalez-Rivas D, Paradela M, Fieira E, Velasco C. (2012). Single-incision video-assisted thoracoscopic lobectomy: initial results. J Thorac Cardiovasc Surg. 2012 Mar;143(3):745-7.
Checking in with Dr. Diego Gonzalez – Rivas and his team in Coruna, Spain – the innovators in single incision thoracic surgery, as Dr. Gonzalez publishes a new report on single incision pneumonectomy.
After speaking with Dr. Raimundo Santolaya last week – I contacted Dr. Diego Gonzalez over at UTCMI in Coruna, Spain to see what he’s been doing since our last contact, and discuss a possible interview in the future.
Last fall, he published another case report on single incision VATS – lobectomy, and since then he has continued to operate and publish reports on his successes. Now he has an upcoming case report on a right-sided single-port pneumonectomy, which was largely held as one of the last frontiers in VATS procedures. (Pneumonectomy by standard VATS, despite being reported in the literature several years ago, remains a relatively uncommon procedure.)
While a common criticism of his work is related to the fact that removing a portion of the lung as large as a lobe, or an entire lung requires a small additional incision at the conclusion of the case – but these criticisms are weak at best – and fail to see the true clinical importance of his continued innovation and investigation in advancing video-assisted thoracoscopic surgery for the benefits of our patients. Ten years from now – single incision VATS will be a common procedure, and Drs. Gonzalez, Fernandez and De la Torre will be the ones responsible.
References: Single port pneumonectomy
Gonzalez-Rivas D, de la Torre M, Fernandez R, Garcia J. (2012). Single-incision video-assisted thoracoscopic right pneumonectomy. Surg Endosc. 2012 Jan 11. [Epub ahead of print – abstract re-posted below]
Abstract
BACKGROUND:The most common approach for Video-assisted thoracoscopic (VATS) lobectomy is undertaken with three or four incisions, including a utility incision of about 3-5 cm. However, major pulmonary resections are amenable by using only a single utility incision. This video shows the technical procedure of a right pneumonectomy by single-incision approach with no rib spreading.
METHODS: A 52-year-old woman was proposed for single-incision VATS resection of a 5-cm right lower lobe adenocarcinoma. A 4-cm incision was made in the fifth intercostal space. We placed a 30-degree, high-definition, 10-mm thoracoscope in the posterior anterior part of the incision. Digital palpation confirmed that the tumor involved the fissure and the posterior portion of the upper lobe, which indicated the need for right pneumonectomy. We inserted the instruments through the anterior part of the utility incision to start the detachment of the right upper lobe by using a harmonic scalpel. The first step was dissecting the inferior pulmonary vein. The hilar structures were exposed by using harmonic scalpel and a long dissector (Fig. 1A). The upper and middle-lobe pulmonary veins were dissected and transected, allowing visualization of truncus anterior, which was then stapled. The inferior pulmonary vein and the intermediate truncus artery were divided, allowing optimal exposure to the main bronchus, which was stapled. The lung was removed in a protective bag by adding 1 cm to the incision, and a systematic lymph node dissection was performed. A single chest tube was placed in the posterior part of the utility incision.
RESULTS: Total surgery time was 210 min. The chest tube was removed on postoperative day 2, and the patient was discharged home on day 4 with no complications.
CONCLUSIONS: Single-port VATS pneumonectomy for selected cases is a feasible procedure, especially when performed from a center with previous experience in double-port VATS approach.
DISCUSSION:Recent advances in surgical and video-assisted techniques have allowed minimally invasive pneumonectomy to be undertaken safely. VATS pneumonectomy is not a new procedure and in fact was initially reported 15 years ago and was felt to result in less postoperative pain and a faster return to normal activities [1]. Despite this, there have been only a few case reports or series published of VATS pneumonectomies [2,3].
Additional References/ Resources
Gonzalez – Rivas, D., Fernandez, R., De la Torre, M., & Martin – Ucar, A. E. (2012). Thoracoscopic lobectomy through a single incision.Multimedia manual cardio-thoracic surgery, Volume 2012. This is an excellent article which gives a detailed description, and overview of the techniques used in single incision surgery. Contains illustrations, full color photos and videos of the procedure.
Gonzalez-Rivas D, Paradela M, Fieira E, Velasco C. (2012). Single-incision video-assisted thoracoscopic lobectomy: initial results. J Thorac Cardiovasc Surg. 2012 Mar;143(3):745-7.
Talking with Sandra Ogawa, ACNP about ‘What to do when the purple pill fails?”
Phoenix, Arizona
During my visit with Dr. Bremner at St. Joseph’s Hospital, I had the pleasure of meeting several members of the thoracic surgery team, including Sandy Ogawa.
Ms. Ogawa is an acute care nurse practitioner specializing in Thoracic Surgery. She initially began working with Dr. Bremner at USC as a nurse coordinator, and has been working with Dr. Bremner since he was a thoracic surgery fellow. After returning to school for her master’s degree – Ms. Ogawa became a nurse practitioner in thoracic surgery.
Since then she has taken on a wide range of duties and responsibilities caring for thoracic surgery patients, with a keen interest in anti-reflux procedures such as the Nissen fundaplication and the Toupet procedure.
One of the things we talked about was her upcoming presentation on proper patient selection and patient referral, or as Ms. Ogawa states, “What to do when the purple pill fails?”
Who should consider surgery for reflux?
The best patients for surgical treatment of reflux are patients who have failed first-line medical treatments such as Nexium (or other proton pump inhibitors.) Patients should explore these options as well as standard medical recommendations such as weight loss, and dietary modification prior to seeking the advice of a surgeon.
Symptoms & Complications of Reflux
Symptoms of GERD are varied and can range from simple heartburn to dysphagia (difficulty swallowing), chest pain, respiratory infections and dental erosion. Uncontrolled gastric reflux has been shown to negatively impact the patient’s quality of life; through interrupted sleep, impaired eating and other activities of daily living.
At St. Joseph’s, Dr Bremner and his colleagues specialize in both of these procedures (Nissen fundaplication and Toupet procedure) as well as re-do procedures for patients with re-current symptoms or re-current hernias after surgery.
Pre-surgical Evaluation: Diagnosis & Testing
Having ‘heartburn’ alone isn’t the only factor to consider prior to undergoing an anti-reflux procedure. The are multiple physiological factors that also help surgeons determine whether surgery is an appropriate treatment, and which surgical procedure is the best surgical option.
As part of their anti-reflux program, all pre-operative evaluation procedures (endoscopy with four quadrant biopsies, barium esophagrams, and manometry are performed in-house. In fact, the department has their own manometry lab, where they read all of their studies (versus sending patients to multiple departments). These tests help determine whether reflux is related to different conditions such as the presence of a hiatal hernia, or a malfunctioning esophageal sphincter. It is also important to rule out other causes of symptoms such as dysphagia such as an esophageal stricture since this condition is treated differently. If there is acid damaged tissue (tissue changes in the esophagus and stomach due to acid erosion), biopsies of the tissue will be taken to rule out Barrett’s esophagus or esophageal cancer.
Guess we’ll have to wait for the rest of Ms. Ogawa’s presentation to hear more.
Additional Resources: Anti-reflux procedures, GERD and treatment strategies
Talking about the clamshell incision in thoracic, cardiac and vascular surgery. Also, soliciting surgical photographs.
The Clamshell Incision
The clamshell incision, also known as a transverse sternotomy, is one of my favorite surgical incisions utilized in thoracic surgery. As surgical procedures become more and more minimally invasive with the use of robotics, and thoracoscopy, we sometimes forget the beauty of the clamshell incision for large-scale thoracic surgeries.
As a frequent observer in the operating rooms of a variety of surgeons employing an array of surgical techniques and operative philosophies, I have a greater opportunity than most to consider the distinct advantages and disadvantages of this surgical approach.
The clamshell incision is shaped like a curved ‘W”, and is typically performed in the anatomic skin / rib groove below the breasts. The surgeon then dissects through the tissue, and intercostal muscles to enter the pleural space bilaterally. It allows greater access than the traditional sternotomy, and has become more popular for bilateral lung transplantation (Durrleman & Massard, 2006). This technique has also been used to salvage lungs in donors that would have otherwise gone unused due to previous sternotomies (Zuin, Marulli, Loy & Rea, 2008).
example of surgical exposure with hemi-clamshell incision
Somewhat ironically, one of the things I like best about this very large surgical incision is the cosmetic results after a successful surgery. Due to the location of anatomical skin folds beneath the breasts, particularly in females – the incision is minimized, and more cosmetically pleasing that standard sternotomy incisions. (There is a nice photo of a healed clamshell incision at this neighboring blog.)
This disadvantages of this incision are obvious; as a large chest incision; longer hospital stays, infection/ poor wound healing, and increased pain but when compared to a similar incision such as a sternotomy, the clamshell may prove superior.
* If you have any medical photographs showing clamshell incisions that you would like featured at cirugia de torax.org, please contact me.
Durrleman, N. & Massard, G. (2006). Clamshell and hemi-clamshell incisions. Multi-media manual of cardio-thoracic surgery, 2006, Issue 0810. Full-text article with discussion of incisions, and intra-operative photos.
Wise, D., Davies, G., Coats, T., Lockey, D., Hyde, J. & Good, A. (2005). Emergency thoracotomy: How to do it. Emergency Medical Journal, 2005;22:22-24. Full-text article with photos showing planned incision and exposure created by the clamshell incision.
Overview of spontaneus pneumothorax and treatment modalities.
There are multiple classifications of pneumothoraces – primary, secondary, iatrogenic, traumatic, tension etc. This article is a limited overview of the most common type(s) of pneumothorax, and methods of treatment.
What are blebs?
The lung is made up of lung tissue itself (consisting of alveoli, bronchi and bronchioles) and a thin, membranous covering called the pleura. This covering serves to prevent inhaled air from travelling from the lung to the area inside the thoracic cavity. ‘Blebs’ are blister-like air pockets that form on the surface of the lung. Bulla (or Bullae for pleural) is the term used for air-filled cavities within the lung tissue.
Who gets/ who has blebs and/or bullae?
Blebs and bullae may be related to an underlying disease process such as emphysema / chronic obstructive pulmonary disease, but they (blebs in particular) may also be found in young, healthy people with no other medical issues. Indeed, the ‘classic’ scenario for a primary spontaneous pneumothorax is a young adult male (18 – 20’s), tall and thin in appearance and no other known medical history who presents with complaints of shortness of breath or dyspnea.
Smoking, and smoking cannabis have been implicated in the development of spontaneous pneumothorax in young (otherwise healthy) patients.
Bullae, or air pockets within the lung tissue are more commonly associated with chronic disease processes such as chronic obstructive pulmonary disease (emphysema). It can be also part of the clinical picture in cystic fibrosis and other lung diseases.
When these blebs rupture or ‘pop’ inhaled air is able to travel from the airways to the thoracic cavity, creating a pneumothorax or lung collapse.
The symptoms of a pneumothorax depend on the amount of lung collapse and the baseline respiratory status of the patient. In young, otherwise healthy patients, the symptoms may be more subtle even with a large pneumothorax. In patients with limited reserve (chronic smokers, COPD, pulmonary fibrosis, sarcoidosis) patients may experience shortness of breath, dyspnea/ difficulty breathing, chest and chest wall pain. With large pneumothoraces or complete collapse of a lung, patients may become cyanotic, or develop respiratory distress.
In cases of pneumothorax caused by external puncture of the lung, or other traumatic circumstances, a patient may develop a life-threatening condition from a tension pneumothorax. This can happen with a simple, primary lung collapse from bleb rupture, but it is uncommon.
How is this treated?
Simple (or first-time) pneumothorax
Oxygen therapy – traditional treatment for small pneumothorax in asymptomatic or minimally symptomatic patients was oxygen via a face mask or non-rebreather. Much of the more recent literature has discredited this as an effective treatment.
Tube thoracostomy (aka chest tube placement) – a chest tube is placed to evacuate air from the thoracic cavity, to allow the lung to re-expand. The chest tube is initially placed to suction until the lung surface heals, and the lung is fully expanded. After a waterseal trial, the chest tube is removed.
Recurrent pneumothorax / other circumstances;
Blebectomy via:
VATS (video-assisted thoracoscopy)
Open thoracotomy or mini-thoracotomy
As we have discussed previously, the VATS procedure / open thoracotomy and mini-thoracotomy are not really stand alone procedures but are the surgical approaches or techniques used to gain entry into the chest. Using a VATS technique involves the creation of one or more ‘ports’ or opening for the use of thoracoscopic surgical tools, and a thoracoscope (or camera.) There are rigid and flexible scopes available; but most thoracic surgeons prefer the rigid scopes for better visibility and control of tissue during the operation[1].
blebs seen during VATS procedure
Open thoracotomy or mini-thoracotomy incisions may be used to gain access to the lung, particularly for resection of bullae (lung volume reduction) surgeries for the treatment of chronic disease.
During this procedure, fibrin sealants may be used. Investigational use of both radio-frequency and other ablative therapies have also been used (Linchevskyy, Makarov & Getman, 2010, Funai, Suzuki, Shimizu & Shiiya 2011**).
Pleurodesis may also be used – in combination with either tube thoracostomy or surgical resection. Pleurodesis can be performed either mechanically, chemically or both. Mechanical pleurodesis is accomplished by irritated the pleura by physical means (such as scratching or rubbing the pleura with the bovie scratch pad or surgical brushes. A chest tube also produces a small amount of mechanical pleurodesis as the tube rubs on the chest wall during patient movement.
Chemical pleurodesis is the instillation of either sterile talc or erythromycin to produce irritation or inflammation of the pleura. With bedside pleurodesis or tube thoracostomy pleurodesis, sterile talc is mixed with lidocaine and sterile water to create a talc slurry. (If you like your patient, carry it in your pocket for 10 – 20 minutes to allow the solution to warm to at least room temperature. This will help reduce the discomfort during instillation.) The mixture should be in a 60cc syringe or similar delivery device – shake briskly before use. The mixture is then instilled via the existing thoracostomy tube. The chest tube is clamped for 30 – 60 minutes (dwell time) and the patient is re-positioned every 10 to 20 minutes. Despite the lidocaine, the talc will produce a burning sensation, so pre-medication is desirable. This procedure has largely fallen out of fashion in many facilities. Post-pleurodesis, pleural inflammation may cause a brief temperature elevation. This is best treated with incentive spirometry, and pulmonary toileting.
Chemical pleurodesis can also be performed in the operating room. Loose sterile talc can be insufflated, or instilled using multiple delivery devices including aerosolized talc. As discussed in previous articles, pleurodesis can also be used for the treatment of pleural effusions.
Special conditions and circumstances related to Pneumothorax:
Catamenial pneumothorax – this a pneumothorax that occurs in menstruating women. It usually occurs on the right-side and is associated with endometriosis, and defects in the diaphragm. A related case study can be viewed here. Several recent studies suggest catamenial pneumothorax may be more common that previously believed and should be suspected in all women presenting with right-sided pneumothorax, particularly if pneumothorax occurs within 48 – 72 hours of menstrual cycle. This may be the first indication of underlying endometrial disease.
[1] Flexible scopes are usually preferred for GI procedures such as colonoscopy, where the camera is inserted into a soft tissue orifice. By comparison, the thoracic cavity with the bony rib cage is more easily navigated with the use of a firm instrument.
** I have contacted the primary authors on both of these papers for more information.
Like all materials presented on this site, this paper is presented for information only. It should not be considered medical advice or treatment. Also, all information provided is generalized information and (outside of clinical case presentations) is not intended to treat of diagnose any disease or condition. If you have questions about the content, please contact us. If you have medical questions, please consult your thoracic surgeon or pulmonologist.
A brief discussion of the variety of surgical approaches used for esophagectomy for esophageal cancer including Ivor Lewis, Transhiatal and minimally invasive techniques.
An esophagectomy is surgical resection of the esophagus. If this includes the upper portion of the stomach (for cancers in the distal third) it is sometimes called an esophagogastrectomy. This procedure is often performed as part of treatment for early stage esophageal cancers. This procedure is technically challenging and requires advanced surgical skill and training in esophageal surgery. The general consensus among surgeons and published literature is that a surgeon needs to perform a minimum of 12- 25 esophagectomies per year to maintain proficiency.
Who does the most esophageal surgeries in the USA? The University of Pittsburgh (UPMC) and Dr. Benny Weksler*.
There are several surgical approaches for this procedure, and the “best” approach is a topic that is widely debated among thoracic surgeons. As technology continues to advance, and newer techniques emerge, esophagectomy/ esophagogastrectomy continues to evolve.
Ivor Lewis Esophagectomy
The Ivor Lewis esophagectomy or the transthoracic approach is considered the ‘Gold standard’ among many thoracic surgeons. Named for the surgeon that popularized this approach in 1946, this surgical procedure is actually a combination of two separate surgical procedures – a laparotomy incision to allow for mobilization of the stomach, and a right-sided thoracotomy for excision and resection of the esophagus. In the modified approach discussed by David & Marshall (2010), the need for patient repositioning in eliminated, allowing for a faster, more efficient operation without sacrificing visibility or accessibility for lymph node dissection. (During the standard approach – the patient is re-positioned after the laparotomy portion of the operation is complete.)
* The presence of metastatic disease drastically changes longevity outcomes, and makes esophagectomy ineffective for cancer treatment.
The main disadvantage is that the Ivor Lewis approach is a big operation (actually two operations) and carries the complications of both a large abdominal operation and a large thoracic procedure (with a thoracotomy.) One of these complications is increased pain. In addition to being burdensome for the patient to endure, the increased pain leads to increased pneumonias, respiratory and other complications due to ineffective pulmonary toileting and limited mobility secondary to this discomfort.)
This procedure is contraindicated in patients who have undergone a previous thoracotomy (due to adhesions). As alluded to above, all surgical resections (Ivor Lewis, Transhiatal and other approaches) are contraindicated in patients with evidence of metastatic disease.
Cerfolio, R. J., Bryant, A. S., Bass, C. S., Alexander, J. R. & Bartolucci, A. A. (2004). Fast tracking after Ivor Lewis esophagogastrectomy.Chest 2004 Oct; 126 (4) 1187 – 94. As the article explains – another advantage of high volume centers is fast-tracking after surgery for a day seven (POD#7) discharge. This also promotes standardization of care which is essential in teaching facilities and other healthcare centers with residents/ students/ frequent staff turnover.
The transhiatal approach was first discussed in the literature in 1933, but fell out of favor for a number of years before making a resurgence in the 1970’s.
In the transhiatal approach, the surgeon still makes two separate incisions – one in the anterior cervical area (neck) and a laparotomy for mobilization of the stomach. The main advantage to this approach is the avoidance of a thoracostomy incision, and a shorter duration of the operation. (The use of a thoracotomy incision is believed to increase the risk of post-operative pulmonary complications). The other advantages of the transhiatal approach are less pain (thoracotomy incision is more painful than cervical approach). This approach also eliminates the possibility of mediastinitis from an anastamotic leak since the anastamosis is not in the thoracic cavity.
However, detractors of this procedure cite the difficulties due to poor visualization of the esophageal tumors during the operation, the increased rate of anastamosis leak and development of post-operative strictures (Barreto & Posner, 2010).
Currently, there are several large randomized studies comparing newer surgical techniques with the Ivor Lewis esophagectomy. The MIRO trial and the TIME trials are on-going. (Enrollment in both of these trials are on-going with more information for interested patients available at clinicaltrials.gov).
There are multiple varieties of approaches for ‘minimally invasive’ esophageal surgery. These procedures are Ivor Lewis or Transhiatal approaches that have been modified by the use of laparoscopic equipment (for the abdominal portion) or thoracoscopic equipment for the transthoracic or transhiatal portion, or a combination of the above. Robot-assisted technologies have also been used in modified approaches to reduce incision size, (thus post-operative pain/ pulmonary complications.) A recent study by Dr. Luketich showed favorable outcomes in a large series of patients undergoing minimally-invasive procedures (link to article abstract below.)
Akiyama, S., Kodera, Y., Koike, M., Kasai, Y., et al. (2001). Small incisional esophagectomy with endoscopic assistance: evaluation of a new technique. Surgery Today, 31 (4) 378 – 382. [no free full text available.] Description of the ‘Akiyama’ approach.
Gao, Y., Wang, Y., Chen, L. & Zhao, Y. (2011). Comparison of open three-field and minimally invasive esophagectomy for esophageal cancer. Interact CardioVasc Thorac Surg 2011, 12: 366 – 369. I would have to argue against the authors contention that the McKeown approach is the preferred open surgical technique of most thoracic surgeons. (The McKeown is a modification of the Ivor Lewis). Surgeons: Care to comment?
Herbella, F. A., & Patti, M. G. (2010). Minimally invasive esophagectomy.World Journal of Gastroenterology,2010 Aug 14; 16 (30) 3811 – 3815.
James D Luketich, MD, Omar Awais, DO*, Manisha Shende, MD*, Neil A Christie, MD*, Benny Weksler, MD*, Rodney J Landreneau, MD, Blair A Jobe, MD*, Ghulam Abbas, MD*, Arjun Pennathur, MD*, Matthew J Schuchert, MD*, Katie S Nason, MD, MPH* University of Pittsburgh, Pittsburgh, PAOutcomes after minimally invasive esophagectomy. Presented at the 131 annual meeting of the American Surgical Association, April 14th – 16th, 2011 in Boca Raton, Fla.
a discussion of Tuberculosis as a surgical disease, with a look at the historical perspectives.
Pneumonectomy, or surgical removal of one entire lung (versus removal of smaller segments of the lung) is a major surgery which is not performed without serious consideration to alternative treatments. Pneumonectomy is indicated as the treatment of choice for otherwise unresectable cancers, as well as serious lung infections such as tuberculosis.
In fact, surgery for tuberculosis (including pneumonectomy) was one of the first set of procedures that helped establish thoracic surgery as a specialty. In the era preceeding the development of antibiotics, there was no effective treatment for tuberculosis – which carried a high mortality rate. Surgical resection of the affected lung was the treatment of choice.
Once antibiotics were established as an effective treatment for this disease, surgery faded into the background – and was primarily reserved for cases complicated by hemoptysis or empyema.
However, in recent years, due to the rise of multi-drug resistance tuberculosis (MDR-TB), surgical resection for the treatment of Tuberculosis has been making a comeback. According to World Health Organization statistics; there were more than 8.8 million cases of TB in 2010. While the death rate has fallen significantly (40%) since 1990 – over 1.4 million people died of TB during that same year. In addition to multi-drug resistant Tuberculosis, there is another subtype called extensively drug resistant tubeculosis (XDR-TB) which is resistant to several drug regimens. (Most cases of non-XDR forms of TB are currently treated with a four drug regimen for several months.)
The emergence of these antibiotic resistant strains have brought us full circle in the surgical management of the disease. Failure of medical therapies leads to a mortality of fifty percent (Kir, et. al (1997). The re-emergence of surgery for tuberculosis is two-fold; surgery is used for both the treatment of active disease and the management of complications from tuberculosis (i.e. removal of dead or damaged lung tissue from previous TB infection.)
A review of the literature surrounding the surgical treatment of tuberculosis explores the modern surgical indications; potential complications and post-operative outcomes. Shiraishi et al. (2008) detail their experiences with surgical resection of several cases of XDR-TB at a Tokyo facility. As explained by Shiraishi, larger operations such as pneumonectomy are preferred over smaller resection procedures because the success of the operation hinges on the ability to remove all of the gross lesions (cavities) or destroyed tissue.
In this article (1997) from Saudi Arabia, Ashour discusses his experiences (from 1985 to 1995) using pneumonectomy to treat post-TB lung destruction.
By reviewing several historical sources, we can review the changing perspectives regarding the treatment of tuberculosis and the indications for surgical resection. While it may be surprising to many readers, the current indicators for surgical resection and pneumonectomy for tuberculosis encourage earlier surgical intervention. In comparison to the late 20th century, where surgery was reserved for cases of extensive lung destruction with gross hemoptysis after years of unsuccessful medical treatment, the development of MDR- TB and XDR-TB provides for ample incentive for surgeons to intervene earlier in the disease process.
Additional References:
Imaging References: Post-pneumonectomy
This article by Padovani et al. (2009) demonstrates examples of normal chest radiographs following pneumonectomy. (article is in French). Post-pneumonectomy films are shown sequentially, from immediately post-operatively, through recovery as the pneumonectomy space fills in. (fig. 1 – 4a.) Figures 4b – 11 show different views of CT scans after pneumonectomy, including views showing partial pleurectomies with mesh placement.
Chandrashekhara SH, Bhalla AS, Sharma R, Gupta AK, Kumar A, Arora R. Imaging in postpneumonectomy complications: A pictorial review. J Can Res Ther 2011;7:3-10 More radiographs following pneumonectomy – depicting potential complications. This is an excellent article reviewing potential early, late and chronic problems after pneumonectomy.
Telzak et. al (1995) explored the phenomenon of multidrug resistant TB in New York City from it’s emergence in the late 1980’s, early 1990’s in this paper, “Multidrug-resistant tuberculosis in patients without HIV infection.” published in the New England Journal of Medicine (1995; 333: 907- 911.) In comparison to other studies, Telzak reported successful outcomes with medical management (at that point in time.)
Adebonojo, S. A., Adebo, O. A., Osinowo, O., & Grillo, I. A. (1981). Management of tuberculosis destroyed lung in Nigeria.Journal of the National Medical Association 1981; 73 (1): 39-42. Report of the results of 20 pneumonectomies performed (1969 – 1979) in cases of moderate to massive hemoptysis. All of these patients were notably sicker than their western counterparts with active symptomology such as night sweats, weight loss, malnutrition, chest pain and varying degrees of hemoptysis. 75% had displayed symptoms for more than five years in spite of receiving several years of antibiotic therapies. Despite this, surgical mortality was low, with acceptable surgical outcomes – giving an interesting historical perspective on this treatment.
Ashour, M. (1997). Pneumonectomy for tuberculosis. Eur J Cardiothorac Surg 1997; 12: 209-213. [full pdf cited in text above.] This study is interesting since the average patient is several years younger than patients in the other studies presented here – demonstrating some of the geographic variability in disease patterns, which is discussed by the author of this article.
Shiraishi, Y., Katsuragi, N., Kita, H., Toishi, M., & Onda, T. (2008). Experience with pulmonary resection for extensively drug resistance tuberculosis. Interact CardioVasc Thorac Surg 2008; 7:1075-1078. [full text pdf link in text].
Yaldiz, S., Gursoy, S., Ucvet, A., & Kaya, S. (2011). Surgery offers high cure rate for drug resistant tuberculosis.Ann Thorac Cardiovasc Surg 2011; 17:143-147. A Turkish study looking at pulmonary resection and chemotherapy for drug resistant TB in 13 patients (from Jan 2003 to Dec 2006). High operative mortality (7.6%) in this study reflects small study size (1 patient). No patients relapsed after surgery.
a selection of full text references talking about robotics and thoracic surgery.
Continuing on our theme of robotic assisted thoracic surgery, here’s a selection of full-text case reports and published reports on thoracic surgery. Some of these stories discuss the more technical aspects of this approach, such as optimal patient positioning, and equipment placement.
Robotic assisted lung resection – an interesting italian/ american study looking at 38 cases (single surgeon experience) from 2001 – 2009. Nicely illustrated. It’s a fascinating study, so I’ve written to the lead author (and surgeon) for more information.
Answers to some of your questions about the basics of Robotic surgery in this re-post of a 2005 article by Dr. Morris.
An article re-post from Medscape, written by a primary care physician (not a surgeon) that gives a nice overview of Robotic Surgery (in general – not specific to thoracic surgery). The article below, from 2005, also talks about the need for increased education for robotic surgery, and the development of specialized training programs. Now – six years later – robotic surgery programs have begun to become more formalized – and we here at Cirugia de Torax are taking a look back at the basics.
Robotic Surgery: Robotic Surgery and Surgical Education
Bishoy Morris
Introduction
The 1990s have witnessed the so-called laparoscopic revolution in which many operations were adapted from the traditional open surgery to the minimal access technique.[1] Shorter hospital stays, reduced postoperative pain, lower incidence of wound infections, and better cosmetic outcomes have made operations, such as laparoscopic cholecystectomy, the standard of care for cholelethiasis.[1-4] Favorable results prompted surgeons to attempt to develop minimally invasive techniques for most surgical procedures. However, many complex procedures (eg, pancreatectomy) proved difficult to learn and to perform laparoscopically due to technical limitations inherent in laparoscopic surgery.[1] For example, the video camera held by the assistant was unstable and gave a limited 2-dimensional vision of the field, and the primary surgeon was forced to adopt awkward positions to operate with straight laparoscopic instruments, limiting maneuvering.[1,2,5] At some point, the growth of the laparoscopic field reached its ostensible plateau, and it seemed that only a new technologic leap could spur further development.
Since the beginning of the 21st century, the emergence of innovative technologies made further advances in minimal access surgery possible. Robotic surgery and telepresence surgery effectively addressed the limitations of laparoscopic and thoracoscopic procedures, thus revolutionizing minimal access surgery.[1,2] Robotic surgery is expected to continue to comprise a growing part of surgery.[6,7] It is envisaged that “almost all surgery can and will be performed by robotic surgery in the future.[5]” Thus, robotic surgery will not only require special training; it will also change the existing surgical training pattern and reshape the learning curve of residents by offering new solutions, such as robotic surgical simulators and robotic telementoring.[1,8]
What Is Robotic Surgery?
A surgical robot is a self-powered, computer-controlled device that can be programmed to aid in the positioning and manipulation of surgical instruments, enabling the surgeon to carry out more complex tasks.[1] Systems currently in use are not intended to act independently from human surgeons or to replace them.[9] Instead, these machines act as remote extensions completely governed by the surgeon and thus are best described as master-slave manipulators.[1] Two master-slave systems have received approval by the US Food and Drug Administration (FDA) and are in use[1,5] — the da Vinci Surgical System (Intuitive Surgical, Mountain View, California)[10,11] and the ZEUS system (Computer Motion, Goleta, California).[1,12] Each system has 2 basic components linked together through data cables and a computer:[1-3,5]
The surgeon’s master consoleis the robot’s user interface that provides the master surgeon with the following functions:
A 3-dimensional view of the surgical field relayed from an endoscopic camera inside the patients body in control of the robot that creates a sense of being “immersed” into the surgical field.
Master manipulators, which are handles or joysticks that the surgeon uses to make surgical movements that are then translated into real-time movements of the slave manipulators docked on the patient. Motion scaling (conversion of large natural movements to ultraprecise micromovements)[13] and tremor filtering increase accuracy and precision of the surgeon’s movements.[14]
A control panel to adjust other functions, such as focusing of the camera, motion scaling, and accessory units.
Patient-side slave robotic manipulators are robotic arms that manipulate the surgical instruments and the camera through laparoscopic ports connected to the patient’s body. The da Vinci system handles surgical instruments with microarticulations near the tip (EndoWrist) that can duplicate motions of the human wrist, including rotation (7 degrees of freedom, ie, the greatest possible motion around a joint).[1,11]
Clinical Applications of Robotic Surgery
Robotic surgery has successfully addressed the limitations of traditional laparoscopic and thoracoscopic surgery,[1-3] thus allowing completion of complex and advanced surgical procedures with increased precision in a minimally invasive approach. In contrast to the awkward positions that are required for laparoscopic surgery, the surgeon is seated comfortably on the robotic control consol, an arrangement that reduces the surgeon’s physical burden.[15] Instead of the flat, 2-dimensional image that is obtained through the regular laparoscopic camera, the surgeon receives a 3-dimensional view that enhances depth perception; camera motion is steady and conveniently controlled by the operating surgeon via voice-activated or manual master controls. Also, manipulation of robotic arm instruments improves range of motion compared with traditional laparoscopic instruments, thus allowing the surgeon to perform more complex surgical movements ( Table 1 ).[1-3,12-14]
Two-dimensional vision of surgical field displayed on the monitor impairs depth perception
Binocular systems and polarizing filters create 3-dimensional view of the field
Movements are counterintuitive (ie, moving the instrument to the right appears to the left on the screen due to mirror-image effect)
Movements are intuitive (ie, moving the control to the right produces a movement to the right on the viewer)
Unstable camera held by an assistant
Surgeon controls camera held in position by robotic arm, allowing solo surgery
Diminished degrees of freedom of straight laparoscopic instruments
Microwrists near the tip that mimic the motion of the human wrist
Surgeon forced to adopt uncomfortable postures during operation
Superior operative ergonomics: surgeon comfortably seated on the control console
Steep learning curve
Shorter learning curve
In a relatively short time, robotic procedures spanning the whole spectrum of surgery have been successfully executed ( Table 2 ).[1,3,16-38] Initial results show that mortality, morbidity, and hospital stay compare favorably to conventional laparoscopic operations.[39] However, only a limited number of randomized, prospective studies that compare outcomes of robotic techniques with conventional methods exist.[40,41] More procedure-specific, randomized trials need to be performed before robotic surgery can find its way into everyday surgical practice.[19,42]
Table 2. Clinical Applications of Robotic Surgery
Field
Operations Performed via Robotic Surgery
Robotic gastrointestinal surgery[1, 16-20]
1997: Himpens et al.[17]— first robotic cholecystectomyAntireflux operations, Heller’s myotomy, gastric bypass, gastrojejunostomy, esophojectomy, gastric banding colectomy, splenectomy, adrenalectomy, and pancreatic resection reported to date
Robotic urologic surgery[21-24]
Radical robotic prostatectomy is the most common operation performed robotically and is gaining widespread recognition in the United States and EuropeNephrectomy and pelvic lymph node dissection also reported
Robotic gynecologic surgery[25-28]
Robotic hysterectomy, salpingo-oophorectomy, and microsurgical fallopian tube reanastomosis
Robotic cardiothoracic surgery[29-34]
Surgical robots allow cardiothoracic surgeons to perform complex cardiothoracic procedures while avoiding the significant morbidity of sternotomy and thoracotomyHundreds of robotic coronary bypasses have been performed to dateMitral valve repairs, atrial spetal defect repair, pericardiectomy, lobectomies, and tumor enucleations
Robotic oncologic surgery[3]
Esophageal tumors, gastric cancer, colon cancer, thymoma, and retromediastinal tumors
Robotic pediatric surgery[35-38]
Pyeloplasty for ureteropelvic junction obstruction, antireflux procedures for gastroesophageal reflux disease, and pediatric congenital heart diseases, such as ligation of patent ductus arteriosus
Limitations of Robotic Surgery
Although rapidly developing, robotic surgical technology has not achieved its full potential owing to a few limitations. Cost-effectiveness is a major issue[43]; 2 recent studies comparing robotic procedures with conventional operations showed that although the absolute cost for robotic operations was higher, the major part of the increased cost was attributed to the initial cost of purchasing the robot (estimated at $1,200,000) and yearly maintenance ($100,000).[43,44] Both factors are expected to decrease as robotic systems gain more widespread acceptance. However, it is conceivable that further technical advances may at first drive prices even higher.[45] Decreasing operative time and hospital stay will also contribute to the cost-effectiveness of robotic surgery.[44]
Other drawbacks to robotic surgery include the bulkiness of the robotic equipment currently in use.[1,7] Lack of tactile and force feedback to the surgeon is another major problem,[1,19] for which haptics (ie, systems that recreate the “feel” of tissues through force feedback) offers a promising, although as yet unrealized, solution.[46,47]
Telepresence Surgery
Telepresence surgery and robotic telementoring are 2 revolutionary applications achieved by linking a robot to a telecommunication system, such as SOCRATES (Computer Motion).[1,3] In telerobotic procedures, the surgeon operates from the surgeon’s console, which is thousands of miles away from the slave robotic arm mounted on the patient; the surgeon’s commands are relayed to the slave manipulator via fiber-optic cables.[1] The first major transatlantic surgery was a telerobotic cholecystectomy performed by surgeons in New York, NY, on a patient in Strasbourg, France, in 2001.[48,49] Since then, many telerobotic operations have been performed. Telepresence surgery allows surgeons to operate wherever their skills are needed without being in direct contact with the patient. Although this virtual surgery has many implications, good and bad, one touted as potentially beneficial is the delivery of surgical care in medically underserved areas.[50,51] However, with a purchase cost around $1 million, a surgical robot is too expensive for places where it is most needed. For example, in Africa the average annual per capita healthcare expenditure is around $6.[52] When finances are not limiting, robotic surgery presents the potential for delivering surgical care to patients who have no direct access to a surgeon. The National Aeronautics and Space Administration (NASA) is exploring the use of surgical robots for emergency surgery on astronauts in a submarine to simulate conditions in space in a project called NEEMO 7.[53] The Pentagon is investing $12 million in a project to develop a “trauma pod” surgical robot to operate on soldiers wounded away from home.[54] A “concept video” extrapolating how such systems can evacuate wounded soldiers under enemy fire and then operate on them is available online.[55]
In telementoring, an expert surgeon guides another surgeon operating miles away; both surgeons “share” the view of the surgical field and control of the robotic system and communicate via microphones. Telementoring can potentially be used for teaching surgical skills to junior surgeons all around the world by expert colleagues.[56-59]
Robotic Surgery and Surgical Education
Despite many technologic leaps, surgical training has stayed more or less unchanged for more than a century. Surgeons in training have always had to gain operative experience through “supervised trial and error” on real patients. This approach makes surgical training completely dependent on the actual case load, prolongs surgical training, and compromises patients’ safety.[1] Robotic surgery will create a new medium for acquisition of surgical skills through simulation of all operations that can be done via the robot. Surgeons can use surgical robots to practice operations on 3-dimensional, virtual-reality visual simulations and soft-tissue models that recreate the textures of human tissues through force feedback (haptics).[60,61] Image-guided simulations will allow surgeons to practice procedures on 3-dimensional reconstructions of the anatomy of the actual patients who they plan to operate on the next day.[62-64] In all of these simulations, trainees can be guided through telementoring. Telepresence surgery has been also successfully used in teaching surgical skills to third-year medical students.[65]
These systems are expected to significantly enhance the learning curve, allowing trainees to acquire surgical skills in a short time while improving patient safety by reducing surgical errors.[1] Ultimately, these applications will be integral to the training and licensing of surgeons and will provide objective means for assessment of surgical skills.[66]
Robotic technology is expected to play an increasingly important role in the future of surgery. However, most residency programs in the United States have not placed adequate emphasis on training in robotic surgery.[1] A survey in 2002 showed that only 23% of surgery program directors have plans to incorporate robotics into their programs.[67] In 2003, another survey by the same group showed that although 57% of surgical residents demonstrated high interest in robotic surgery, the majority (80%) did not have a robotic training program in their institutions.[68] A few academic centers have developed formal didactics to train teams in robotic surgery.[69]
Ensuring competency to perform robotic procedures is left to individual hospitals. It is expected that as formal training in robotic surgery develops, more standardized credentials will be required to obtain robotic surgical privileges.[45,70]
Conclusion
Although still in its infancy, robotic surgery is a cutting-edge development in surgery that will have far-reaching implications. While improving precision and dexterity, this emerging technology allows surgeons to perform operations that were traditionally not amenable to minimal access techniques. As a result, the benefits of minimal access surgery may be applicable to a wider range of procedures. Safety has been well established, and many series of cases have reported favorable outcomes. However, randomized, controlled trials comparing robotic-assisted procedures with laparoscopic or open techniques are generally lacking.
Telerobotic surgery stands out as a way of delivering surgical care to patients who have no direct access to a surgeon; however, costs are prohibitive to the spread of such technology to underserved areas that need it most. Even in the United States, surgical robots are mainly available in large academic centers. The issues of cost, technical drawbacks, and clinical effectiveness need to be resolved before robotic procedures can become mainstream, everyday surgical procedures.
New technologies, such as virtual reality, haptics, and telementoring, can powerfully ally with surgical robots to create a new medium for acquisition and assessment of surgical skills through simulation of all operations that can be done via the robot. Performance of robotic procedures requires specialized training. However, the majority of residency programs in the United States do not provide formal training in robotic surgery skills. Students, residents, and residency programs should strive to keep up with this new development in surgical technology that is likely to reshape the way we practice surgery.
Gomez G. Emerging Technology in surgery: informatics, electronics, robotics. In: Sabiston Textbook of Surgery. 17th ed. Philadelphia, Pa: Elsevier Saunders; 2004.
Ballantyne GH. The pitfalls of laparoscopic surgery: challenges for robotics and telerobotic surgery. Surg Laparosc Endosc Percutan Tech. 2002;12:1-5. Abstract
Ballantyne GH. Robotic surgery, telerobotic surgery, telepresence, and telementoring. Review of early clinical results. Surg Endosc. 2002;16:1389-1402. Abstract
Darzi SA, Munz Y. The impact of minimally invasive surgical techniques. Annu Rev Med. 2004;55:223-237. Abstract
Hashizume M, Tsugawa K. Robotic surgery and cancer: the present state, problems and future vision. Jpn J Clin Oncol. 2004;34:227-237. Abstract
Marohn MR, Hanly EJ. Twenty-first century surgery using twenty-first century technology: surgical robotics. Curr Surg. 2004;61:466-473. Abstract
Camarillo DB, Krummel TM, Salisbury JK Jr. Robotic technology in surgery: past, present, and future. Am J Surg. 2004;188:2S-15S. Abstract
Di Lorenzo N, Coscarella G, Faraci L, Konopacki D, Pietrantuono M, Gaspari AL. Robotic systems and surgical education. JSLS. 2005;9:3-12. Abstract
Stylopoulos N, Rattner D. Robotics and ergonomics. Surg Clin North Am. 2003;83:1321-1337. Abstract
Ballantyne GH, Moll F. The da Vinci telerobotic surgical system: the virtual operative field and telepresence surgery. Surg Clin North Am. 2003;83:1293-1304. Abstract
Marescaux J, Rubino F. The ZEUS robotic system: experimental and clinical applications. Surg Clin North Am. 2003;83:1305-1315. Abstract
Prasad SM, Prasad SM, Maniar HS, Chu C, Schuessler RB, Damiano RJ Jr. Surgical robotics: impact of motion scaling on task performance. J Am Coll Surg. 2004;199:863-868. Abstract
Moorthy K, Munz Y, Dosis A, et al. Dexterity enhancement with robotic surgery. Surg Endosc. 2004;18:790-795. Abstract
Smith WD, Berguer R, Rosser JC Jr. Wireless virtual instrument measurement of surgeons’ physical and mental workloads for robotic versus manual minimally invasive surgery. Stud Health Technol Inform. 2003;94:318-324. Abstract
Hubens G, Ruppert M, Balliu L, Vaneerdeweg W. What have we learnt after two years working with the da Vinci robot system in digestive surgery? Acta Chir Belg. 2004;104:609-614.
Brunaud L, Bresler L, Ayav A, et al. Advantages of using robotic Da Vinci system unilateral adrenalectomy: early results. Ann Chir. 2003;128:530-535. Abstract
El-Hakim A, Tweari A. Robotic prostatectomy — a review. MedGenMed. 2004;6:20.
Spaliviero M, Gill IS. Robot-assisted urologic procedures. Semin Laparosc Surg. 2004;11:81-88. Abstract
Phillips CK, Taneja SS, Stifelman MD. Robot-assisted laparoscopic partial nephrectomy: the NYU technique. J Endourol. 2005;19:441-445. Abstract
Guillonneau B, Cappele O, Martinez JB, Navarra S, Vallancien G. Robotic assisted, laparoscopic pelvic lymph node dissection in humans. J Urol. 2001;165:1078-1081. Abstract
Advincula AP, Falcone T. Laparoscopic robotic gynecologic surgery. Obstet Gynecol Clin North Am. 2004;31:599-609. Abstract
Falcone T, Goldberg J, Garcia-Ruiz A, Margossian H, Stevens L. Full robotic assistance for laparoscopic tubal anastomosis: a case report. J Laparoendosc Adv Surg Tech A. 1999; 9:107-113. Abstract
Margossian H, Falcone T. Robotically assisted laparoscopic hysterectomy and adnexal surgery. J Laparoendosc Adv Surg Tech A. 2001;11:161-165. Abstract
Marchal F, Rauch P, Vandromme J, et al. Telerobotic-assisted laparoscopic hysterectomy for benign and oncologic pathologies: initial clinical experience with 30 patients. Surg Endosc. 2005;19:826-831. Abstract
Nifong LW, Chitwood WR, Pappas PS, et al. Robotic mitral valve surgery: a United States multicenter trial. J Thorac Cardiovasc Surg. 2005;129:1395-1404. Abstract
Chitwood WR Jr. Current status of endoscopic and robotic mitral valve surgery. Ann Thorac Surg. 2005;79:S2248-2253. Abstract
Argenziano M, Oz MC, Kohmoto T, et al. Totally endoscopic atrial septal defect repair with robotic assistance. Circulation. 2003;108(suppl1):II191-194.
Wimmer-Greinecker G, Deschka H, Aybek T, Mierdl S, Moritz A, Dogan S. Current status of robotically assisted coronary revascularization. Am J Surg. 2004;188:76S-82S. Abstract
Morgan JA, Ginsburg ME, Sonett JR, Argenziano M. Thoracoscopic lobectomy using robotic technology. Heart Surg Forum. 2003;6:E167-169. Abstract
Melfi FM, Menconi GF, Mariani AM, Angeletti CA. Early experience with robotic technology for thoracoscopic surgery. Eur J Cardiothorac Surg. 2002;21:864-868. Abstract
Bentas W, Wolfram M, Brautigam R, et al. Da Vinci robot assisted Anderson-Hynes dismembered pyeloplasty: technique and 1 year follow-up. World J Urol. 2003;21:133-138. Abstract
Lorincz A, Langenburg S, Klein MD. Robotics and the pediatric surgeon. Curr Opin Pediatr. 2003;15:262-266. Abstract
Suematsu Y, Del Nido PJ. Robotic pediatric cardiac surgery: present and future perspectives. Am J Surg. 2004;188(suppl):98S-103S.
Cannon JW, Howe RD, Dupont PE, Triedman JK, Marx GR, del Nido PJ. Application of robotics in congenital cardiac surgery. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2003;6:72-83. Abstract
Talamini MA, Chapman S, Horgan S, Melvin WS; The Academic Robotics Group. A prospective analysis of 211 robotic-assisted surgical procedures. Surg Endosc. 2003;17:1521-1524. Abstract
Morino M, Beninca G, Giraudo G, Del Genio GM, Rebecchi F, Garrone C. Robot-assisted vs laparoscopic adrenalectomy: a prospective randomized controlled trial. Surg Endosc. 2004;18:1742-1746. Abstract
Cadiere GB, Himpens J, Vertruyen M, et al. Evaluation of telesurgical (robotic) NISSEN fundoplication. Surg Endosc. 2001;15:918-923. Abstract
Delaney CP, Lynch AC, Senagore AJ, Fazio VW. Comparison of robotically performed and traditional laparoscopic colorectal surgery. Dis Colon Rectum. 2003;46:1633-1639. Abstract
Morgan JA, Thornton BA, Peacock JC, et al. Does robotic technology make minimally invasive cardiac surgery too expensive? A hospital cost analysis of robotic and conventional techniques. J Card Surg. 2005;20:246-251. Abstract
Lotan Y, Cadeddu JA, Gettman MT. The new economics of radical prostatectomy: cost comparison of open, laparoscopic and robot assisted techniques. J Urol. 2004;172:1431-1435. Abstract
Lowenfels AB. Robotics. Highlights of the American College of Surgeons 90th Annual Clinical Congress. Medscape CME Conference Coverage. Available at: http://www.medscape.com/viewarticle/498575 Accessed September 7, 2005.
Bethea BT, Okamura AM, Kitagawa M, et al. Application of haptic feedback to robotic surgery. J Laparoendosc Adv Surg Tech A. 2004;14:191-195. Abstract
Tholey G, Desai JP, Castellanos AE. Force feedback plays a significant role in minimally invasive surgery: results and analysis. Ann Surg. 2005;241:102-109. Abstract
Marescaux J, Leroy J, Gagner M, et al. Transatlantic robot-assisted telesurgery. Nature. 2001;413:379-380. Abstract
Marescaux J, Rubino F. Robot-assisted remote surgery: technological advances, potential complications, and solutions. Surg Technol Int. 2004;12:23-26. Abstract
Marescaux J, Leroy J, Rubino F, et al. Transcontinental robot-assisted remote telesurgery: feasibility and potential applications. Ann Surg. 2002;235:487-492. Abstract
Anvari M, McKinley C, Stein H. Establishment of the world’s first telerobotic remote surgical service: for provision of advanced laparoscopic surgery in a rural community. Surg Laparosc Endosc Percutan Tech. 2002;12:17-25. Abstract
Peters DH, Elmendorf AE, Kandola K, Chellaraj G. Benchmarks for health expenditures, services and outcomes in Africa during the 1990s. Bull World Health Organ. 2000;78:761-769. Abstract
Bove P, Stoianovici D, Micali S, et al. Is telesurgery a new reality? Our experience with laparoscopic and percutaneous procedures. J Endourol. 2003;17:137-142. Abstract
Mendez I, Hill R, Clarke D, Kolyvas G. Robotic long-distance telementoring in neurosurgery. Neurosurgery. 2005;56:434-440.
Latifi R, Peck K, Satava R, Anvari M. Telepresence and telementoring in surgery. Stud Health Technol Inform. 2004;104:200-206. Abstract
Marescaux J, Rubino F. Telesurgery, telementoring, virtual surgery, and telerobotics. Curr Urol Rep. 2003;4:109-113. Abstract
Suzuki S, Suzuki N, Hayashibe M, et al. Tele-surgical simulation system for training in the use of da Vinci surgery. Stud Health Technol Inform. 2005;111:543-548. Abstract
Satava RM. Virtual reality, telesurgery, and the new world order of medicine. J Image Guid Surg. 1995;1:12-16. Abstract
Weiss H, Ortmaier T, Maass H, Hirzinger G, Kuehnapfel U. A virtual-reality-based haptic surgical training system. Comput Aided Surg. 2003;8:269-272. Abstract
Hattori A, Suzuki N, Hayashibe M, Suzuki S, Otake Y, Tajiri H, Kobayashi S. Development of a navigation function for an endosocopic robot surgery system. Stud Health Technol Inform. 2005;111:167-171. Abstract
Kaufmann C, Rhee P, Burris D. Telepresence surgery system enhances medical student surgery training. Stud Health Technol Inform. 1999;62:174-178. Abstract
Ro CY, Toumpoulis IK, Ashton RC Jr, et al. A novel drill set for the enhancement and assessment of robotic surgical performance. Stud Health Technol Inform. 2005;111:418-421. Abstract
Donias HW, Karamanoukian RL, Glick PL, Bergsland J, Karamanoukian HL. Survey of resident training in robotic surgery. Am Surg. 2002;68:177-181. Abstract
Patel YR, Donias HW, Boyd DW, et al. Are you ready to become a robo-surgeon? Am Surg. 2003;69:599-603.
Chitwood WR Jr, Nifong LW, Chapman WH, et al. Robotic surgical training in an academic institution. Ann Surg. 2001;234:475-484. Abstract
Ballantyne GH, Kelley WE Jr. Granting clinical privileges for telerobotic surgery. Surg Laparosc Endosc Percutan Tech. 2002;12:17-25. Abstract
[Bishoy Morris, MBBCH (Hons), Primary Care Physician, Ministry of Health, Assiut, Egypt; Member, Editorial Board, MedGenMed “The Learning Curve”. Email: beshoyso@yahoo.com
Disclosure: Morris Bishoy, MBBCH (Hons), has disclosed no relevant financial relationships.
an in-depth look at video-assisted thoracoscopy for decortication of advanced empyema.
In a previous series of posts discussing a recent paper presented by a group of Australian pulmonologists, we debated the use of VATS for decortication of advanced empyemas versus medical treatments. Today, I would like to talk more about the VATS decortication procedure itself. This procedure is performed to remove infected material (pus) from the thoracic cavity so the lung can re-expand.
when fully encapsulated as seen in this ct scan may be difficult to distinguish from lung abscess – but note the compressed lung, which is a characteristic of empyema.
In advanced empyema, a tough, fibrous layer (or peel) forms around the lung and prevents full re-expansion. (This peel has the appearance and texture of rubbery chicken skin.)
thick pleural removed during decortication
In these cases, decortication (or peel removal) is necessary for full recovery.
VATS decortication of a loculated empyema
If the peel isn’t removed, the lung will remain compressed and infection can easily recur. In VATS surgery, several ports are used (small 2cm incisions) versus a larger thoracotomy incision. This isn’t always possible; if the infection is severe, or surgeons are unable to free the lung through the smaller incisions. Sometimes surgeons have to convert to open surgery intra-operatively. However, VATS is preferable for patients, (if possible). Smaller incisions mean less injury, less pain leading to fasting healing, and a shorter hospital stay.
advanced empyema requiring open thoracotomy for decortication
Asian Cardiovasc Thorac Ann 2010;18:337–43. Thoracic empyema in high-risk patients: conservative management or surgery? Bar I, Stav D, Fink G, Peer A, Lazarovitch T, Papiashvilli M. Limited study of 119 patients showing benefit in both groups of patients with surgery used as primary management strategy in clinically unstable patients. (Increased mortality in this limited study of surgical interventions versus medical management can be attributed to the fact that surgery was used as a last resort in the sicker, more debilitated patients by the authors descriptions).
Metin M, Yeginsu A, Sayar A, Alzafer S, Solak O, Ozgul A, Erkorkmaz U, Gürses A. Treatment of multiloculated empyema thoracis. Singapore Med J. 2010, Mar 51(3): 242-6. Comparison of VATS, open surgery and conventional treatment for empyema. Authors recommend VATS for first line treatment.
Discussion of a case report by Gonzalez, Paradela, Garcia & Dela Torre (2011) of a lobectomy by single incision thoracoscopic surgery.
Since there’s been quite a bit of interest in single-port thoracoscopic surgery (SITS) here at Cirugia de Torax.org – I’ve added information about SITS lobectomy. British surgeons, Rocco et. al had previously reported the outcomes of several wedge resections by uni-port (SITS) back in 2004 but this is the first case report that I’ve seen for lobectomies via this technique*.
Gonzalez et al. in Coruna, Spain published a case report of a lobectomy by SITS. The authors note that they have performed three cases by this technique at the time of article submission (November 2010).
As expected, the authors reported decreased post-operative pain and parathesias when using this technique. They also reported that while visibility is more limited with this approach, they feel that it is less problematic for surgeons already accustomed to, and familiar with double port lobectomies. This approach, in their experience, is best used for lower lobe lesions due to difficulties accessing and maneuvering for bronchial resection for upper lobectomies.
* If you’ve seen other published reports – please send the citations to the site.
Update: 25 July 2011
I contacted Dr. Gonzalez to inquire about his surgical experiences since the publication of the article this past March. Dr. Gonzalez reports that he and his colleagues (Dr. Mercedes De la Torre and Dr. Fernandez) have continued to practice SITS for lobectomies and other thoracic procedures, and that he is now using it for the majority of his cases.
Dr. Gonzalez states that many of his patients are discharged earlier (POD 2 or 3) and are experiencing less post-operative pain. He is planning future studies to demonstrate this.
Gonzalez D., Paradela M., Garcia J. & De la Torre M. (2011). Single-port video-assisted thoracoscopic lobectomy. Interact Cardiovasc Thorac Surg. 2011 Mar;12(3):514-5. Epub 2010 Dec 5. (free full-text article with photographs).
Rocco, G., Martin-Ucar, A. & Passera, E. (2004). Uniportal VATS wedge pulmonary resections.Ann Thorac Surg 2004;77:726-728. (free full text aricle with color photographs).
Chen et. al discuss their experience with single incision thoracoscopic surgery (SITS) in the treatment of spontaneous pneumothorax in this Taiwanese study.
A study from Taiwan (April 2011) highlights the surgeons’ experience using single incision thoracoscopic surgery (SITS) for the treatment of spontaneous pneumothorax. While the study is small – involving 30 patients, with just ten patients receiving treatment via single incision thoracoscopy, it’s a useful study in demonstrating that SITS is not only possible but feasible for uncomplicated thoracic procedures.
The major advantage of using this procedure in the spontaneous pneumothorax population is the low level of underlying thoracic disease, or co-morbidities necessitating conversion to VATS or open surgery. In general, true spontaneous pneumothoraces occur in younger patients (teens and twenties) in the absence of other conditions such as infection, emphysema or effusion. The benefits of using this procedure in such a young, mobile population is reduced pain, and a speedier recovery – and returning these patients to work/ life faster, with less post-operative limitations.
As the authors noted, a consistent obstacle to widespread adoption of this surgical technique is the lack of specialized surgical instruments. This has also plagued single incision laparoscopy to some extent, with several minor modifications being made by practicing surgeons to overcome these problems, primarily of positioning several instruments thru a single port*. This is more problematic in thoracic surgery than general surgery due to patient positioning. (In general surgery the patient is usually laying supine, allowing for a flat surface).
Example of single incision laparoscopy for cholecystectomy
In thoracic surgery, the patient’s side lying positioning puts the operator at greater disadvantage, with gravity working against the surgeon. As mentioned in a previous post – there is a commercial port of multiple instruments available, however it is costly, unwieldly and requires larger incisions (making SITS more of a mini-thoracotomy). The other mechanical problem is the instruments themselves – when placed in a single incision, care has to be taken to prevent the instruments from obstructing the movements of each other. The authors were able to overcome this obstacle thru practice, but suggest needed modifications to existing instruments.
Despite frequently cited concerns about visibility with this technique, in the article (and confirmed by my own observations in the operating room), properly done single incision thoracoscopy offers the same visibility as multi-port (VATS) thoracoscopy. (See the original article full text for photos of procedure illustrating visibility.)
More recently, (June 2011) Berlanga & Gigirey in Caceres, Spain reported the use of SITS for spontaneous pneumothorax in 13 patients. They reported similar findings, and came to the same conclusions as Chen et. al. However, these researchers used the commercially available port and reported satisfactory results.
There is a place for single incision thoracoscopy within thoracic surgery. However, it will take continued research to further delineate its role, and surgical innovation to adapt the current instrumentation for more effective and surgeon friendly use.
Berlanga, L. A. & Gigirey, O. (2011). Uniportal video-assisted thoracic surgery for primary spontaneous pneumothorax using a single–incision laparoscopic surgery port: a feasible and safe procedure. Surg Endosc. 2011 Jun;25(6):2044-7. Epub 2010 Dec 7. Full text article not available for link (paid article).
A discussion of and link to the Yan et. al (2011) article, “Improving survival rates after surgical management of pleural malignant mesothelioma: an australian institutional experience” as part of a series of posts on mesothelioma and extrapleural pneumonectomy (EPP).
A recent study by Yan et al. (2011) conducted at the Royal Prince Alfred Hospital in Sydney, Australia does more than look at the outcomes of the aforementioned treatment for malignant pleural mesothelioma. This study, involving 540 patients, over 25 years also gives us a primer on the evolving treatment therapies for this condition. As newer treatment therapies emerged, these therapies were given to eligible patients, starting with extrapleural pneumonectomy itself, in 1994 and extending to include both radiotherapy and chemotherapy. Chemotherapy consisted of a combination of pemtrexed, carboplatin and cisplatin. While this alters the results significantly it also provides for an interesting introspective on the treatment of malignant pleural mesothelioma.
This study is noteworthy for both this reason, and as a study looking at a larger set of patients than many of the other studies on this topic.
Study Design: consecutive, non-randomized.
Patient population: 540 patients; organized into two groups for statistical analysis. Group I – 270 patients (consecutive patients from March 1984 to September 1999.) Group II – consecutive patients September 1999 to Jan 2008. As the authors noted, due to the rarity of this condition in Australia, it took 25 years to recruit 540 patients for treatment.
Patient characteristics: the vast majority were male (455 patients) with a mean age of 66 (+/- 11 years). 315 patients with right-sided disease, the remaining 225 with left-sided disease.
Disease subtypes:
235 patients with epithelial subtype, 212 with sarcomoid/ biphasic (type determined by tissue pathology)
Treatments received:
69 patients had extrapleural pneumonectomy
269 patients received pleurectomy/ decortication
202 patients received pleurodesis
62 patients received post-operative radiotherapy starting 8 to 12 weeks after surgery. This treatment was added in 2002.
65 of the patients received adjunctive chemotherapy
Notably, as mentioned above, there was a distinct difference in the treatment allocation for groups I and II due to changing treatment protocols, and the development of new therapies. While 22% of patients in group II received EPP, only 5% of patients in group I received the same surgical procedure.
Treatment strategies were also limited by patient factors; namely the patient’s physical condition / functional status as being considered able to withstand the proposed treatment therapy. As mentioned in a previous post, extrapleural pneumonectomy is an extensive surgical procedure which requires significant patient reserves and pre-existing functional abilities for anticipated recovery. In frail or debilitated patients, (as defined by criteria set forth by Yan et. al) EPP was not attempted. Some of these patients received either pleurectomy with decortication. In patients deemed too fragile to withstand either of these procedures, a talc pleurodesis (either by VATS or tube thoracostomy) was performed as a palliative procedure. Unsurprisingly, the patients receiving palliative treatment options had shorter median survival periods.
Results:
18 patients died in the perioperative period, including 3 EPP patients.
Median follow-up period for the study was ten months. At the time of follow-up the majority of patients (433 patients, 80%) had died with a median survival time of nine months for group I (range 0 – 115 months).
In group II, the median survival time was 13 months. (range 0 – 72 months).
Long term survival by group:
Group I Group II
1 year 35% 50 %
2 year 16% 22%
3 year 9 % 12%
5 year 2 % 9 %
These five-year survival rates highlight the importance of continued studies for the advancement of treatment therapies for this condition.
Factors associated with greater survival:
In reviewing their research, the authors were able to identify four independent factors that increased the likelihood of survival in this population. (See original article for discussion in further depth.)
1. Yan et. al found that the epithelial subtype was more favorable for patient survival, and that this subtype was more common in the patients in group II.
3. Patients who received EPP had improved survival compared to patients who received other treatments. However, this also reflects a selection bias, since the patients who were eligible for EPP had better pre-operative functional status than patients who received other treatments.
4. Premetrexed chemotherapy – patients who received this chemotherapy regimen had greater survival.
blog author’s note:
Despite dismal five year survival rates for treatment of malignant pleural mesothelioma by a multitude of treatment methods, extrapleural pneumonectomy (with adjuvant chemotherapy) appears to be the most effective cytoreductive surgery for this condition. ( As noted in related posts, HITHOC is an emerging therapy that combines the principles of both.) We will continue to follow research in these areas for the treatment of malignant pleural mesothelioma and invite the experts to add their comments.
A brief description of pulmonary metastasectomy (lung resection for metastatic disease) with a limited review of recent literature.
Pulmonary metastasectomy is a medical term used to indicate surgical resection or removal of a metastatic lung lesion. This terminology reflects the presence of an underlying non-lung primary cancer. This terminology can sometimes be confusing for patients; particularly as the surgical procedure itself is unchanged (from lung procedures for other lung lesions.)
In lay person’s terms; this is also sometimes called “cherry-picking[1]”.
The Procedure: Lung Resection
Usually, patients undergo the standard VATs or open wedge resection used for other primary lung lesions, to remove the cancerous tissue. The amount and type of surgery depends on the location and size of the lung lesion, so in some cases patients have bigger procedures such as lobectomies or pneumonectomies for this condition.
The reason for delineating a difference in terminology is related to long-term outcomes and adjuvant treatment strategies. This means that the accompanying treatments such as chemotherapy or radiation are different for different underlying diseases (ie. primary lung tumor versus metastatic disease from different area.)
For example:
Patient A has a wedge resection for a primary lung tumor, which turns out to be a bronchiogenic adenocarcinoma during intra-operative pathologic reporting (the lesion is sent to the pathologist during surgery & we wait for his report before completing the rest of the surgery.) The best treatment for this is a lobectomy, which is completed while the patient is still in the operating room.
Patient X has a history of colon cancer which was previously treated with surgical resection of the colon, and chemotherapy. X has been doing well but a recent CT scan shows a lesion in the right lower lobe of his lung, with no other lesions seen. Since Mr. X has a history of colon cancer – this lesion may be a metastatic colon lesion – and the adjuvant treatment, as well as the post-operative prognosis is very different.
How do we know who would benefit from pulmonary metastasectomy? (A brief look at the published literature)
1. The International Registry of Lung Metastases (IRLM): (the link is to a nice article explaining more about the history of registry and initial results). The registry was first started in 1990, and as the name suggests, this is an international registry that was created to track the outcomes of patients with lung metastases. By tracking this data, we are able to better understand which treatment therapies are useful/ life-saving and which treatments aren’t, according to patient disease characteristics (i.e patient with breast cancer and a lung lesion may fare differently than a patient X from our example above.)
The initial data from the registry actually came from fifty years of chart reviews, starting from 1945 to 1995. This study, by Pastorino, is considered the Hallmark for pulmonary metastases. All other studies build on this body of work, to either confirm, refute or expand on their findings.
Other researchers have looked at this as well: (this is just a small sample of recent research findings)
2. Zabaleta et. al (April 2011) published an article in Cirugia Espanola, “Review and update of prognostic factors in lung metastasis surgery” which nicely explains their findings. Zabaleta and his team compiled data on ten years worth of patients (146 total) and determined that the most important factors for predicting outcomes were: age of patient, disease free interval (after initial disease treated), the number of lung nodules and the size of these nodules. This study confirms the original findings.
Unsurprisingly, the patients that did the best (lived the longest and least or re-operations for more lesions) were the patients aged 41 – 79 who had long periods before the lesion appeared, with a solitary nodule less than one centimeter in size. Clear surgical margins were not determined to be statistically significant (due to low-frequency of positive margins in study population) but all of the patients with positive surgical margins failed to survive the study period (only nine cases with + margins).
Patient Population: The majority of the patients in this study (54.8%) had colo-rectal primaries, but there was a sizable sarcoma primary population
(12.3%) as well as several other primary types which adds to the generalizability of the study.
Patient outcomes: 38 patients (26%) developed recurrent lung lesions after lung surgery – with a mean time to recurrence of 18 months (range of 3 to 60 months). I would have liked to have known which primaries were responsible in the recurrence group, since certain cancers are more aggressive than others. Overall mean survival was 67 months, with a five-year survival rate of 52.4% While the authors mention the poor prognosis of sarcoma, it would have been nice if they could have broken down the survival statistics better by primary cancer type – as the authors attribute survivability by cancer factors rather than type (i.e. sarcoma usually has multiple mets).
3. A Japanese study published this winter in the Annals of Thoracic Surgery looking at colorectal patients with metastatic liver metastasis who underwent pulmonary metastasectomy (lung resection). Study population was small (19 patients) despite a long study period (1992 – 2006) but findings were interesting with a five-year survival rate of 60%.
Patient population: 77 patients who had 122 surgeries involving 273 nodules – this gives you a bit more of an idea how sarcoma can differ from other cancers (more lung mets – multiple nodules). Study period was a chart review of patients referred to thoracic surgery from 1990 to 2006.
Findings: number of metastatic lesions less important than resectability, meaning “Were they able to get it all?” This; [complete resectability] was the greatest predictor of survival – and 34.7 % of patients in this study survived 90 months (then investigators stopped looking). Mean survival was 36 months.
This is just a fraction of the literature out there, but all of these studies were well-written, and freely available without subscriptions. There are a couple of interesting studies that are awaiting journal publication – so I will try to update this article once they are published.
[1] The term cherry picking referred to the patients that are selected to undergo surgery for their metastatic lesions. Usually the patient has only one or two metastatic lesions – which can essentially be surgically removed or ‘plucked out’. This procedure is less feasible / successful in patients with multiple, bilateral lesions.
Extrapleural pneumonectomy for malignant mesothelioma
Extrapleural Pneumonectomy (EPP) is a radical operation in which the entire lung, and tissues of the lung space (pleura, diaphragm and pericardium) are removed. This is done as part of a cancer operation, often for an aggressive cancer called malignant mesothelioma. During cancer operations, surgeons have to remove all or as much cancer tissue as possible, including microscopic cells that are not visible to the surgeon at the time of surgery. Any tissue that is left behind may have cancer cells which will continue to grow, and spread. Due to the location of the cancer cells (in the lining), surgeons have to remove more tissue than if the cancer was centered in the lung itself. This includes replacing the diaphragm with a synthetic patch during surgery.
Mesothelioma is named after the cells it affects. These mesothelial cells make up the “linings” of the body cavities. For this reason, mesothelioma can affect other areas of the body, in the linings of the abdomen called the peritoneum, the pericardium (the lining around the heart), and most commonly, the pleura.
Inside the chest, coating the chest wall is a thin lining tissue called the pleura. The interior area of the rib cage and chest are thus called the pleural cavity. When mesothelial cancer cells invade this fragile tissue layer, it is called pleural mesothelioma, which is different from peritoneal mesothelioma. (Peritoneal mesothelioma affects the peritoneal cavity, or abdominal cavity.)
Not everyone is a candidate for this surgery. Due to the radical nature of this procedure, patients need to have good pulmonary function and overall functional status prior to surgery. (The patient is going to lose one whole lung during this procedure, so patients that are already oxygen dependent / bedridden or otherwise debilitated won’t be able to tolerate this procedure.) The best patients for this surgery (the patients who will have the best outcomes/ receive the most benefits from surgery) are patients with good functional status (able to perform normal activities of daily living) with earlier stages of the disease. In these patients – this surgery can extend their lives significantly. In patients with more advanced (stage III/ stage IV) disease, the surgery will make them live longer (months) but the quality of life may be worse post-operatively.
Prior to consideration for extrapleural pneumonectomy (or any other treatment) the doctors will want to definitively diagnose (prove the diagnosis through tissue biopsy) and do preliminary staging. (Final staging occurs after the operation when further tissue / lymph node biopsies are evaluated by the pathologist).
Preliminary staging and pre-operative evaluation is the process to try to figure out how much cancer is present (has it spread?) and whether the patient can tolerate a large operation. Mediastinoscopy; a surgical procedure to look at mediastinal lymph nodes (lymph nodes behind the sternum or breast bone), PET scans and blood for tumor markers help determine how much cancer is present. The tumor markers also help the oncologists figure out which chemotherapy drugs will work the best.
Pre-operative testing is looking at lung function, to see how well the patient will do with only one lung. Cardiac testing may be done as well since surgery can be stressful to the heart.
If the disease is controllable with surgery, and the surgeon thinks the patient can withstand surgery – the surgeon will consult with an oncologist about the timing of surgery and adjuvant treatments (chemotherapy/ radiation).
Even with radical surgery, the prognosis for malignant pleural mesothelioma is poor, but improves with combination therapies (surgery with chemotherapy/ radiation.) Currently, surgeons are investigating the use of cytoreductive hyperthermic chemotherapy (HIPEC/ Hithoc) for treatment of pleural based mesothelioma. (Previous studies by Dr. Paul Sugarbaker has shown this treatment to be effective with advanced abdominal cancers including malignant peritoneal mesothelioma.) We will discuss HIPEC further on a future post.
There are numerous studies looking at extrapleural pneumonectomy for treatment of malignant pleural mesothelioma. The links below is just a small sampling.
1. Extrapleural pneumonectomy for malignant pleural mesothelioma (2005) – Argote- Greene, Chang, and Sugarbaker. (Note: this article was co-authored by Dr. David Sugarbaker, Department of Thoracic surgery, Brigham Womens & Children’s, not Dr. Paul Sugarbaker, developer of HIPEC. I am going to attempt to contact Dr. Davis Sugarbaker for commentary for the site since he is the expert on this topic, so hopefully I’ll be able to update the site with his post in the future.
2. Radical surgery for malignant pleural mesothelioma – Japanese study comparing results for EPP versus pleurectomy / decortication. The main points to take away from this study is that stage of disease has a huge impact on prognosis, and outcomes after surgery. (The patients with stage I and II that underwent EPP did fairly well.)
3. Review of 83 cases of EPP – (2009) French study which unintentionally highlights the potential complications of surgery of this magnitude(almost 40% had major complications and had a re-operative rate of almost fifteen percent.)
the development and application of single-port thoracoscopic surgery, (or the lack there of.)
Right now, single incision scopic surgery (laparoscopic, generally*) is in all the literature. This is a minimally invasinve technique using only one port (or incision) for access to the surgical area (usually the abdomen).
I’ve seen it performed by several general surgeons as part of my travels for BogotaSurgery.org and read the literature surrounding it, but hadn’t heard much about it’s close kin, single port thoracoscopic surgery, though I’d seen it performed during a trip to Cartagena early last year. At the time, I immediately noticed the difference in technique in the operating room (it’s not something you miss) but the surgeon performing the procedure just sort of shrugged, and went back to work, a “Yeah, well.. I do this all the time sort of thing.”
Since that trip, I’ve talked to several thoracic surgeons about this technique, and they all agreed; that due to limited visibility and maneverability, it was a procedure with “limited applications”. But it didn’t sound like any of them had attempted it, or knew much on the subject.
Since ‘limited applications’ describes many surgical techniques, I decided to go to the literature, and see what has been published on the topic.
Hmm.. Not much.
An article from two Spanish surgeons dating to 2009. It’s a well written article with a decent amount of subjects (24) for the treatment of spontaneous pneumothorax. They mention one of the adaptations required is use of the Coviden multi-station system to hold instruments – this is a silly piece of equipment that costs about a thousand dollars. I know that in general surgery, several surgeons have adapted a sterile surgical glove for the same purpose. Since use of this costly but specialized piece of rubber also requires an even bigger incision – I hope these surgeons have since moved on to the sterile glove technique. In this study, length of stay and amount of post-operative pain were not greatly reduced, which was a little surprising.
Jutley, Khalil and Rocco published a paper in 2005 in the European Journaol of Cardiothoracic Surgery on the same technique for spontaneous pneumothorax with 16 patients having uniport surgery (versus 19 in the standard three port group) with positive findings of reduced pain, and less residual neuralgias.
An Italian group reported similar positive findings (compared to Jutley, et. al) in 2008 on a similar sized group/ population (28 patients uniport versus 23 ‘traditional’ 3 port). They also reported a minimum of problems with the uniport technique.
So, three published studies (there are probably more, but this is what I could find over at Pubmed) with minimum of fuss or problems… So, why isn’t there more single incision thoracoscopic surgery? Where are the surgeons performing this technique? Maybe I’m just not talking to enough thoracic surgeons, or the right thoracic surgeons..
I’ll get back to you on this.
* This laparoscopic technique goes by the anacronym: SILS for single-incision laparoscopic surgery. It is also called uni-port (uniportal) laparoscopy and it has both it’s champions and detractors.
Discussion of treatment goals, and patient centered care for Malignant pleural effusions. This is the first in a series of articles on lung cancer, and lung surgery topics. Originally posted at our sister site.
Not all conditions are curable, and not all treatments are curative. Some treatments are based on improving quality of life, and alleviating symptoms. This is a hallmark of patient centered care – doing what we can to make the patient feel better even when we can’t ‘fix’ or cure the underlying disease. No where is this more evident than in the treatment of malignant effusions.
By definition, a Malignant Effusion is the development of fluid in the fluids related to an underlying (and sometimes previously undiagnosed) malignancy. Malignant effusions can be seen with several different kinds of cancers, most commonly lung and breast cancers. The development of a malignant effusion is a poor prognostic sign as it is an indicator of metastasis to the pleural tissue/ space.
The development of a malignant effusion usually presents with symptoms of shortness of breath, and difficulty breathing. While the treatment of the underlying cancer may vary, the primary goal of treatment of an effusion is palliative (or symptom relief). The best way to relieve symptoms is by removing the fluid.
This can be done several ways – but each has its own drawbacks.
Thoracentesis:
The fluid can be drawn out with a needle (thoracentesis) either bedside or under fluroscopy. This procedure is quick, and can be performed on an out-patient basis, in a doctor’s office, or in radiology.
The potential drawbacks with this treatment strategy are two-fold:
1. There is a chance that during the procedure, the needle will ‘poke’ or ‘pop’ the lung, causing a pneumothorax (or collapse of the lung). This then requires a chest tube to be placed so the lung can re-expand while it heals. However, if the procedure is performed uneventfully, (like it usually does) the patient can go home the same day.
2. The other complication – is rapid re – accumulation – since you haven’t treated the underlying cause, but have only removed the fluid. This also happens when the cause of the effusion (nonmalignant) is from congestive heart failure. This means the fluid (and symptoms of shortness of breath) may return quickly, requiring the patient to return to the hospital – which is hard of the patient and their family.
Video- Assisted Thoracoscopy: (VATs)
Malignant effusions can also be treated by VATS – this is a good option if we are uncertain of the etiology (or the reason) for the effusion. While all fluid removed is routinely sent for cytopathology (when removed during surgery, thoracentesis or chest tube placement) – but cytopathology can be notoriously inaccurate with false negative reports, because the diagnosis is dependent on the pathologist actually seeing cancer cells in the fluid. However, during the VATs procedure – the surgeon can take tissue samples, and photos along with fluid for diagnostic testing. This is important because I have had cases in the operating room (VATS) where the surgeon actually sees the tumor(s)** with the camera but the fluid comes back as negative.
** in these cases, we send biopsies of the tumor tissue – which is much more accurate and definitive.
But a VATS procedure requires an operation, chest tube placement and several days in the hospital.
Chest tube placement:
Another option is chest tube placement – which also requires several days in the hospital..
During both chest tube placement and VATS, a procedure called pleurodesis can be performed to try to prevent the fluid from re-accumulating.
But what if we know it’s a malignant effusion? What are the other options for treatment?
Catheter based treatments: (aka PleurX style catheter, or Heimlich valve)
(note: catheter means a small tube – a foley catheter is the type used to drain urine, but other types are used for many things – even an IV is a catheter.)
One of the options used in our practice was pleur X (brand) catheter placement. This catheter was a small flexible tube that could be placed under local anesthesia – either in the office or the operating room – as an ambulatory procedure. After some patient teaching, including a short video, most family members felt comfortable emptying the catheter every two or three days at home, to prevent fluid re -accumulation (and allowing the patient to continue normal activities, at home.)
PleurX catheter placement is preferred in many cases due to ease of use, and patient convenience. The Heimlich valve is messier – as it tends to leak, and harder for patients to hide under clothing.
Sometimes a visiting nurse would go out and empty the catheter, and in several cases, patients would come to the office, where I would do the same thing – it was a nice way to relieve the patient’s symptoms without requiring hospitalization, and several studies have shown that repeated drainage often caused spontaneous pleurodesis (fluid no longer accumulated.) We would then take the catheter out in the office.. Now, like any procedure, there is a chance for problems with this therapy as well, infection, catheter can clog, etc..
But here’s another study, showing that even frail patients benefit from home-based therapy – which is important when we go back and consider our original treatment goals:
-Improving quality of life
-Relieving symptoms
In the article, the authors used talc with the catheters and then applied a Heimlich valve, which is another technique very similar to pleurX catheter placement. (Sterile talc is used for the pleurodesis procedure – which we will talk about in more detail in the future.)