information about the upcoming VATS symposium in Cambridge, UK – with featured speakers Dr. Diego Gonzalez Rivas and Ian Hunt.
Another conference/ educational announcement for all residents, fellows and interested thoracic surgeons. This course is sponsored by the United Kingdom’s National Health Service and is being held in Cambridge, UK at Papworth Hospital this November. There is parallel content for nurses and other thoracic surgery personnel.
Internationally known Spanish surgeon Dr. Diego Gonzalez Rivas as well as native surgeon Mr. (Dr.) Ian Hunt of St. George’s Hospital in London, will be part of the faculty teaching this course.
Dr. Gonzalez Rivas will be discussing single port surgery in addition to performing a live case on the second day of the symposium.
Mr. Hunt will be discussing how to perform a total lymphadenectomy, as well as lymphadenectomies on more complicated cases.
Additional speakers will be discussing topics including issues in thoracic anesthesia, management of bleeding (in VATS and other minimally invasive surgery), and managing other operative complications.
the Babe Ruth of thoracic surgery continues his winning streak; and Dr. Benny Weksler heads south to the University of Tennessee. Kudos to both of these fine surgeons!
It’s another home run for Dr. Gonzalez Rivas as he and his team perform a single port (uni-port) thoracoscopic lobectomy with under local anesthesia, as reported by a recent story, “Operan un tumor e pulmón con una sola incisión y anestesia local” by Raul Romar in La Voz de Galicia.
Dr. Gonzalez Rivas demonstrates uniportal VATS
The answer is International collaboration and sharing of ideas
Dr. Gonzalez Rivas is used to sharing his ideas. After all, he spends a considerable amount of time traveling the world doing just that; sharing information about and teaching surgeons how to perform the single port thoracoscopic technique. But that doesn’t mean that he does find time to learn from his peers during his travels.
The article above highlights the importance of this international collaboration as it details how Dr. Gonzalez Rivas began to consider applying a local anesthesia approach to the single port surgical technique after talking (and visiting) surgeons in Taiwan and China.
Once he found the perfect candidate, he was ready to implement local anesthesia into his single port approach.. The rest, as they say – is now headed for the Annals of Thoracic Surgery.
Click here for English translation (note translation is not exact).
Dr. Benny Weksler, our own American (via Brazil) superstar surgeon recently made the move to the University of Tennessee. Dr. Weksler made the move in November of 2013 and is now settling in to his new position as Chief of Thoracic Surgery for the University of Tennessee (UT) Health Science Center and UT – Methodist.
Dr. Weksler, one of the United States most prominent thoracic surgeons, particularly in the area of esophageal surgery reports that he has big plans for the UT health system and the thoracic surgery department.
Big Plans for UT and the city of Memphis
These plans include a lung cancer screening program targeting vulnerable populations in Memphis including the uninsured/ underinsured, African-Americans (who are disproportionately affected) and smokers.
Related: Dr. Weksler talks about smoking cessation
Minimally invasive techniques for esophageal surgery
He has also started a new minimally invasive esophageal surgery program for esophageal cancer and reports “that there is almost an epidemics of squamous cell carcinoma of the esophagus” which is something tha was more rare in his previous practice in Pittsburgh, Pennsylvania.
Dr. Weksler and his colleagues are putting together a multi-disciplinary treatment plan to try to get these patients to a complete evaluation with a surgeon, an oncologist, and a radiation oncologist to provide patients with comprehensive, multi-faceted and coördinated care.
“The Surgeon Speaks” – Dr. Weksler talks about robotic surgery in this 2009 Jefferson University publication.
As a former Memphis resident, I want to say, “Welcome to the mid-south.. Hope you find time in your busy schedule to enjoy Beale Street, visit the Pink Palace and tour Graceland.. On behalf of all current Memphians, we are glad you are here.”
*This article was written by the author of this post.
in the operating room with Dr. Diego Gonzalez Rivas for single port thoracoscopic (uniportal) surgery.
Hilar mass resection using single port thoracoscopy with Dr. Diego Gonzalez – Rivas
K. Eckland & Andres M. Neira, MD
Instituto Nacional de Cancerlogia
Bogota, Colombia
Surgeon(s): Dr. Diego Gonzalez Rivas and Dr. Ricardo Buitrago
Dr. Diego Gonzalez Rivas demonstrates single port thoracoscopy
Case History:
59-year-old female with past medical history significant for recurrent mediastinal mass previously resectioned via right VATS. Additional past medical history included prior right-sided nephrectomy.
Pre-operative labs:
CBC: WBC 7230 Neu 73% Hgb:14.1 Hct 37 platelets 365000
Pt 12.1 / INR1.1 PTT: 28.3
Diagnostics:
Pre-operative CT scan: chest
edited to preserve patient privacy
Procedure: Single port thoracoscopy with resection of mediastinal mass and lymph node sampling
After review of relevant patient history including radiographs, patient was positioned for a right-sided procedure. After being prepped, and draped, surgery procedure in sterile fashion. A linear incision was made in the anterior chest – mid clavicular line at approximately the fifth intercostal space. A 10mm port was briefly inserted and the chest cavity inspected. The port was then removed, and the incision was expanded by an additional centimeter to allow for the passage of multiple instruments; including camera, grasper and suction catheter.
Dr. Gonzalez Rivas and Dr. Ricardo Buitrago at National Cancer Institute
The chest cavity, pleura and lung were inspected. The medial mediastinal mass was then identified.
As previously indicated on pre-operative CT scan, the mass was located adjacent and adherent to the vessels of the hilum. This area was carefully dissected free, in a painstaking fashion. After freeing the mediastinal mass from the hilum, the remaining surfaces of the mass were resected. The mass was fixed to the artery pulmonary and infiltrating it) . The mass was removed en-bloc. Care was then taken to identify, and sample the adjacent lymph nodes which were located at stations (4, 7 and 10).
Following removal of the tumor and lymph nodes, the area was re-inspected, and the lung was re-inflated. A 28 french chest tube was inserted in the original incision, with suturing of the fascia, subcutaneous and skin layers.
closing the single port incision
Hemostasis was maintained during the procedure with minimal blood loss.
Patient was hemodynamically stable throughout the case, and maintained appropriate oxygen saturations. Following surgery, the patient was awakened, extubated and transferred to the surgical intensive care unit.
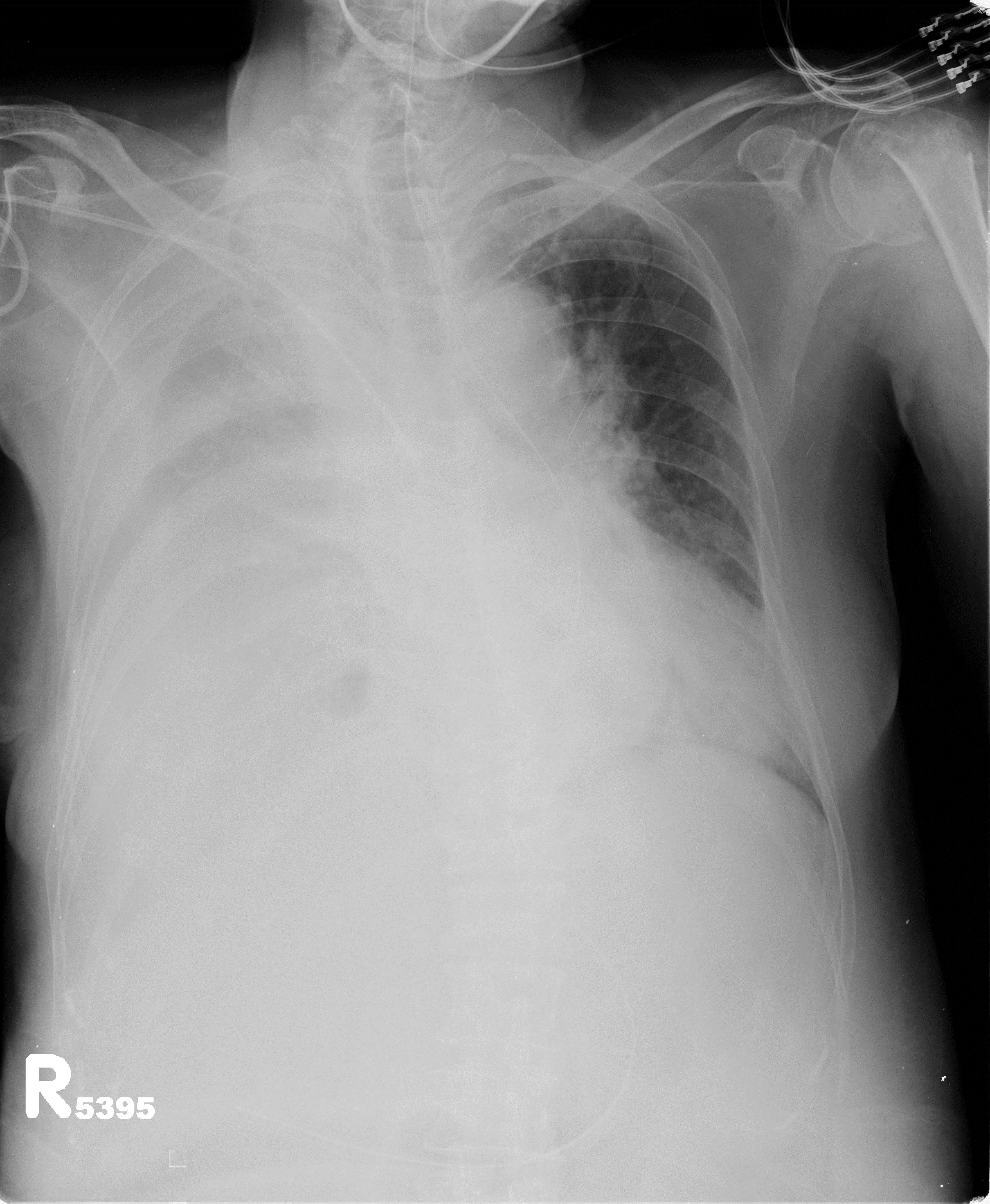
Post-operative: Post-operative chest x-ray confirmed appropriate chest tube placement and no significant bleeding or pneumothorax.
Immediate post-operative film (chest tube visible)
Patient did well post-operatively. Chest tube was discontinued on POD#2 and discharged home.
PA & LAT films on post-operative day 2
Discussion: Since the initial published reports of single-port thoracoscopy, this procedure has been applied to an increasing range of cases. Dr. Gonzalez and his team have published reports demonstrating the safety and utility of the single-port technique for multiple procedures including lobectomies, sleeve resections, segmentectomies, pneumonectomies and mediastinal mass resections. Dr. Hanao Chen (Taiwan) has reported several successful esophagectomies using this technical, as well as bilateral pleural drainage using a unilateral single-port approach.
Contrary to popular perception, the use of a single-port versus traditional VATS procedures (three or more) is actually associated with better visibility and accessibility for surgeons. Surgeons using this technical have also reported better ergonomics with less operating fatigue related to awkward body positioning while operating.
The learn curve for this surgical approach is less than anticipated due to the reasons cited above, and has been cited at 5 to 20 cases by Dr. Gonzalez, the creator of this approach.
The main limitations for surgeons using this technique is often related to anticipated (but potentially unrealized) fears regarding the need for urgent conversion to open thoracotomy. In reality, many of the complications that may lead to urgent conversion, such as major bleeding, are manageable thoracoscopically once surgeons are experienced and comfortable with this approach.
Dr. Gonzalez and his colleagues have reported a conversion rate of less than 1% in their practice. Subsequent reports by Dr. Gonzalez and his colleagues have documented these findings.
Other barriers to adoption of this technique are surgeon-based, and may be related to the individual surgeon’s willingness or reluctance to adopt new techniques and technology. Many of these surgeons would be surprised by how this technique mimics open surgery.
The successful adoption of this technique by numerous thoracic surgery fellows shows the feasibility and ease of learning single-port thoracoscopy by surgeons interested in adopting and advancing their surgical proficiency in minimally invasive surgery.
The benefits for utilizing this technique include decreased length of stay, decreased patient discomfort and greater patient satisfaction.
References/ Additional Readings
Bertolaccini, L., Rocco, G., Viti, A. & Terzi, A. (2013). Surgical technique: Geometrical characteristics of uniportal VATS. J. Thorac Dis. 2013, Apr 07. Article from thoracic surgeons at the National Cancer Institute in Naples, Italy explains how the geometric advantages of uniportal VATS improves visibility and spatial perception over traditional VATS, and mimics open surgery.
Calvin, S. H. Ng (2013). Uniportal VATS in Asia. J Thorac Dis 2013 Jun 20. Article discussing the spread of uniportal techniques in Taiwan, China and other parts of Asia.
Chen, Chin-Hao, Lin, Wei-Sha, Chang, Ho, Lee, Shih-Yi, Tzu-Ti, Hung & Tai, Chih-Yin (2013). Treatment of bilateral empyema thoracis using unilateral single-port thoracoscopic approach. Ann Thorac Cardiovasc Surg 2013.
Gonzalez Rivas, D., Fieira, E., Delgado, M., Mendez, L., Fernandez, R. & De la Torre, M. (2013). Surgical technique: Uniportal video-assisted thoracoscopic lobectomy. J. Thorac Dis. 2013 July 4.
Gonzalez Rivas, D., Delgado, M., Fieira, E., Mendez, L. Fernandez, R. & De la Torre, M. (2013). Surgical technique: Uniportal video-assisted thoracoscopic pneumonectomy. J. Thorac Dis. 2013 July 4.
Rocco, G. (2013). VATS and uniportal VATS: a glimpse into the future. J. Thorac Dis. 2013 July 04. After coming across several articles by Dr. Gaetano Rocco, and actively pursuing several other publications by this Italian thoracic surgeon, I have become increasingly convinced that Gaetano Rocco, along with Dr. Gonzalez Rivas is one of the world’s leading innovators in thoracic surgery. Hopefully, cirugia de torax will be able to catch up to Dr. Rocco at some point for an in-depth discussion.
Rocco G. Single port video-assisted thoracic surgery (uniportal) in the routine general thoracic surgical practice. Op Tech (Society of Thoracic and Cardiovascular Surgeons). 2009;14:326–335.
Rocco G, Khalil M, Jutley R. Uniportal video-assisted thoracoscopic surgery wedge lung biopsy in the diagnosis of interstitial lung diseases. J Thorac Cardiovasc Surg. 2005;129:947–948.
5 / Video-assisted thoracic surgery lobectomy: 3-year initial experience with 200 cases. Gonzalez D, De la Torre M, Paradela M, Fernandez R, Delgado M, Garcia J,Fieira E, Mendez L. Eur J Cardiothorac Surg. 2011 40(1):e21-8.
6 / Single-port Video-Assisted Thoracoscopic Anatomical Resection: Initial Experience. Diego Gonzalez , Ricardo Fernandez, Mercedes De La Torre, Maria Delgado, Marina Paradela, Lucia Mendez. Innovations.Vol 6.Number 3. May/jun 2011. Page 165.
writing about Dr. Diego Gonzalez Rivas and the other living legends in thoracic surgery and connecting people to the world of thoracic surgery
Readers at Cirugia de Torax have certainly noticed that there are numerous articles regarding the work of Dr. Diego Gonzalez Rivas. This week in particular, after a recent thoracic surgery conference and an afternoon in the operating room – there is a lot to say about the Spanish surgeon.
It’s also hard to escape that fact that I regard him in considerable awe and esteem for his numerous contributions to thoracic surgery and prolific publications. I imagine that this is similar to how many people felt about Drs. Cooley, Pearson or Debakey during their prime.
Making thoracic surgery accessible
But the difference is Dr. Diego Gonzalez Rivas himself. Despite the international fame and critical surgical acclaim, he remains friendly and approachable. He has also been extremely supportive of my work, at a time when not many people in thoracic surgery see the necessity or utility of a nurse-run website.
After all, the internet is filled with other options for readers; CTSnet.org, multiple societies like the Society of Thoracic Surgeons (STS), and massive compilations like journal-based sites (Annals of Thoracic Surgery, Journal of Thoracic Disease, Interactive Journal of Cardiothoracic Surgery).
But the difference between Cirugia de Torax and those sites is like the difference between Dr. Gonzalez Rivas and many of the original masters of surgery: Approach-ability and accessibility.
This site is specifically designed for a wider range of appeal, for both professionals in thoracic surgery, and for our consumers – the patients and their families. Research, innovation, news and development matters to all of us, not just the professionals in the hallowed halls of academia. But sometimes it doesn’t feel that way.
Serving practicing surgeons
For practice-based clinicians, and international surgeons publication in an academia-based journal requires a significant effort. These surgeons usually don’t have research assistants, residents and government grants to support their efforts, collect their data and clean up their grammar. Often English is a second or third language. But that doesn’t mean that they don’t make valuable contributions to their patients and the practice of thoracic surgery. This is their platform, to bring their efforts to their peers and the world.
Heady aspirations
That may sound like a lofty goal, but we have readers from over a 110 countries, with hundreds of subscribers along with over 6,000 people with Cirugia de Torax directly on their smart phone. Each month, we attract more hits and more readers.
Every day, at least 200 people read “Blebs, Bullae and Spontanous Pneumothorax”. Why? Because it’s a concise article that explains what blebs are, how a pneumothorax occurs and how it’s treated. Another hundred people usually go on to read the accompanying case report about blebectomy, for similar reasons. There are links for more information, CT scans and intra-operative photos included, so that people can find exactly what they need with a minimum of effort.
Avoiding ‘Google overload’
With the massive volume of information available on the internet, high-quality, easily understood, applicable information has actually become even more difficult for patients to find than ever before. Patients spend hours upon hours browsing through academic jargon, commercial websites and biased materials while attempting to sift through the reams of information for pertinent and easily understandable information. There is also a lot of great material out there – so we provide links to reputable sites, recommend well-written articles and discuss related research.
Connecting patients to surgeons
We also provide patients with more information about the people they are entrusting their bodies, their hopes and their lives to. It’s important that they know about the Dr. Benny Wekslers, the Dr. Hanao Chens, and the Dr. Diego Gonzalez Rivas out there.
Update: June 2019
After multiple reader requests from this site, we have launched a service to assist readers in pursuiting minimally invasive thoracic surgery, uniportal surgery, HITHOC and other state-of-the-art thoracic surgery procedures with the modern masters of thoracic surgery. We won’t talk a lot about this on the site, but we do want readers to know that we are here to help you. If you are wondering what surgery costs like with one of the world’s experts – it’s often surprisingly affordable.
If you are interested in knowing more, please head to our sister site, www.americanphysiciansnetwork.org or send an email to kristin@americanphysiciansnetwork.org.
Keeping it ‘real’
Looking over the shoulder of Dr. Gonzalez Rivas in the operating room
As much as I may admire the work and the accomplishments of Dr. Gonzalez-Rivas – it’s important not to place him on a pedestal. He and his colleagues are real, practicing surgeons who operating on regular people, not just heads of state and celebrities. So when we interview these surgeons and head to the OR, it’s time to forget about the accolades, the published papers and the fancy titles. It’s time to focus on the operations, the techniques, the patients and the outcomes because ‘master of thoracic surgery’ or rural surgeon – the operation and patient are all that really matters.
Discussing Dr. Joseph Coselli and ‘the cowboys of cardiac surgery’ along with some of our own heros of thoracic surgery here at Cirugia de Torax.
There’s a great article in this month’s Annals of Thoracic Surgery, by Dr. Joseph Coselli, from Texas Heart Institute and the Michael DeBakey Department of Surgery at Baylor. His article, entitled,” My heros have always been cowboys” is more than just a title torn from the song sheets of Willie Nelson. It’s a look back at both the pioneers of cardiac surgery and his own experiences as a cardiac surgeon. He also discusses the role of surgeons, and medical practitioners in American society in general and the promises we make to both society at large and our patients.
Here at Cirugia de Torax, I’d like to take a moment to look back at the surgeons that inspired and encouraged me in this and all of my endeavors. Some of these surgeons knew me, and some of them didn’t – but their encouragement and kindnesses have spurred a career and life that have brought immense personal and professional satisfaction.
Like Dr. Coselli, I too, took inspiration from the likes of Dr. Denton Cooley. But our stories diverge greatly from there. I never met Dr. Cooley and I probably never will. But it was a related story, from my former boss (and cardiothoracic surgeon), Dr. Richard Embrey that led to an email to Dr. Cooley himself. My boss had too trained under Dr. Cooley, Dr. Debakey and the Texas Heart Institute, the citadel of American heart surgery. Then, somehow, along the way – Dr. Embrey stopped to work at our little rural Virginia hospital. We were the remnants of a larger Duke cardiothoracic program but we were a country hospital all the same.
While I learned the ins and outs of surgery from Dr. Embrey (and Dr. Geoffrey Graeber at West Virginia University) on a day-to-day basis, I was also weaned on the folklore of cardiothoracic surgery – stories of the giants of history, like the ones mentioned in Dr. Coselli’s article, as well as local Duke legends who occasionally roamed the halls of our tiny ICU and our two cardiothoracic OR suites; Dr. Duane Davis, Dr. Shu S. Lin and Dr. Peter Smith. While never working side-by-side, Dr. D’Amico’s name was almost as familiar as my own. As the sole nurse practitioner in this facility, without residents or fellows, there was no buffer, and little social divide in our daily practice. Certainly, this changed me – and my perceptions. I asked the ‘stupid’ questions but received intelligent and insightful answers. I asked even more questions, and learned even more..
These opportunities fed my mind, and nurtured my ambitions. Not to be a physician or a doctor, but to learn as much as possible about my specialty; to be the best nurse possible in my field. It also nurtured a desire to share these experiences, and this knowledge with my peers, my patients and everyone else who ever had an interest.
It was that tiny little email, a gracious three-line reply from Dr. Cooley himself that made me realize that I didn’t have to rely on folklore and second-hand stories to hear more. That’s critical; because as we’ve seen (here at Cirugia de Torax) there are a quite of few of “Masters of thoracic surgery” or perhaps future giants that haven’t had their stories told. Dr. Coselli and his fellow writers haven’t written about them yet.. So I will.
Sometimes I interview famous (or semi-famous) surgeons here, but other times, I interview lesser-known but equally talented/ innovative or promising surgeons. All of them share similar traits; dedication and love for the profession, immense surgical talent and proficiency and sincere belief in the future of technology of surgery.
So, let’s hope that it won’t take forty more years for these surgeons to be recognized for their contributions to thoracic surgery in the way that Cooley, DeBakey and Crawford are heralded in cardiac surgery.
Case report with video of SITS (single incision thoracoscopic surgery) repair of diaphragm defect in a case of hepatic hydrothorax resulting from liver cirrhosis with Dr. Chih-Hao Chen, MAckay Memorial Hospital, Taiwan
Case Report: Single incision thoracoscopic repair of diaphragmatic defect in a patient with hepatic hydrothorax
Dr. Chih-Hao Chen, Thoracic Surgeon MAckay Memorial Hospital, Taiwan
Dr. Chen, Thoracic Surgeon
Clinical History:
Patient is an elderly woman who was admitted after a motor-vehicle accident with a traumatic fracture of the humerus and femoral neck. She was brought to our ED immediately and was intubated due to acute respiratory failure.
Subsequent Chest radiograph showed diffuse opacity in right hemithorax and concomitant fracture in left side humerus and femoral neck. Attempt for tapping of the pleural effusion showed clear in nature.
According to previous medical records, she had no relevant history. She was admitted to ICU for further evaluation and management.
Fluid analysis in emergency department showed transudate.
LFTS: Total Bilirubin 2.7 mg/dL AST 116 ALT 68 Albumin 2.3 g/dL Direct Bilirubin H 1.1 mg/dL
Chem panel: BUN 83 mg/dL Creatinine 1.6 mg/dL K 3.2 mEq/LNa 144 mEq/L
Chest radiograph on admission showed a massive right-sided pleural effusion.
Chest radiograph on admission
For symptomatic control, the physician performed intermittent thoracentesis. Because the traumatic site is left aspect of the trunk ( fracture in left side humerus and left side femoral neck ) and right side effusion was very clear.
Hepatic hydrothorax was suspected. Later peritoneal scan confirmed the diagnosis.
Peritoneal scan
The scan showed left side pleural space was sparring from radioisotope. Direct communication between right side pleural cavity and the abdomen. The diagnosis is confirmed with such findings.
CT scans are not diagnostic for this condition, and were not indicated for her other injuries. Therefore, we did not arrange CT scan of the chest / abdomen.
Abdominal ultrasound showed moderate to massive ascites. Along with hepatic encephalopathy, moderate to massive ascites, prolonged PT/PTT, low albumin, higher bilirubin, the extent of cirrhosis is Child’s class C.
Operative Procedure: Single incision thoracoscopic repair of a diaphragmatic defect. Theoretically, with SITS, the wound can be very tiny. However, in our experience (fifteen total cases to date), diaphragm surgery through single port may be a bit difficult because we did not know where the defect is. We have to inspect very carefully and to search for the defect where the fluid came out. In this case, we made one small wound around 2 cm in length at the 6th ICS along the anterior axillary line.
Repair of the diaphragmatic defect was performed using silk suture similar to that used to repair inguinal hernias. Intra-operatively, the defect was 2 -3 mm in diameter.
At the conclusion of the procedure, using the original incision, we placed one Fr.24 chest tube to monitor the drainage and may consider chemical pleurodesis if the drainage persists. The operative procedure was accomplished within 30 minutes.
Post-operative Chest Radiograph
Post-operative condition of the chest film showed near complete resolution of the effusion and lung re-expansion was complete.
Pathology/ Fluid Cytology: fluid analysis and peritoneal scan showed communication between peritoneal space and right side pleural space confirming pre-operative diagnosis. No tissue specimens were taken during this procedure.
Discussion:
Hepatic hydrothorax is the development of a pleural effusion in a patient with liver disease in the absence of cardiopulmonary pathology, making it a diagnosis of exclusion in many cases. It can occur in patients with and without ascites and may be the first presenting symptom in patients with undiagnosed liver disease. Similar to catamenial pneumothorax; hepatic hydrothorax is predominantly a right-sided disease. This is due to an anatomic gutter or diaphragmatic defect that occurs, and allows the passage of material or fluid from the abdominal cavity into the pleural space. This can be seen and identified on peritoneal studies(Peritoneal scan) like the study showed in our case study above. (Similar pathologies can occur in related conditions such as renal failure related hydrothorax due to this defect). Such defect is usually identified in the tendon part of the diaphragm. Peritoneal scan can confirm there is communication between the abdominal cavity and the pleural space. However, the definite location, size and number of defects can not been identified by the scan alone. Thoracoscopic inspection is the only method to search for such defect(s).
Video-assisted thoracoscopic surgery (VATS) has been shown to be a safe and effective method of treating this condition, by allowing surgeons to correct the defect, and thus prevent recurrence (Saito et al. 2012). The cure rate varied greatly in the literature. The key is whether the defect can be repaired. For one to two obvious defects, direct suture repair usually cured the disease. (the cure rate more than 80%) However, for some undetectable defects or defects with fenestration type, the cure rate is very low, ( around 30-50% ). Alternative strategies have to be considered in such condition, such as tissue glue, abrasion pleurodesis, mesh interposition and using sclerosing agents(OK432, bleomycin, Minocin, talc, etc). This is in distinct contrast to the numerous non-surgical drainage procedures such as thoracentesis, which removes accumulated fluid but does not correct the underlying pathology. However, the hallmark of this condition, liver failure predisposes patients to complications such as bleeding, infection and poor wound healing. These risks are one of the primary reasons treatment was often limited to drainage procedures prior to the popularization of lower risk VATS procedures. In the past, patients with Child’s class C liver cirrhosis are basically not proper surgical candidates because of extremely high mortality/morbidity rate. In recent experience of single-port approach, some patients with Child B and C are still safe with minimal postoperative complications. The advance of these minimally invasive technologies such as uni-port thoracoscopy permits fewer and more limited incisions which is believed to further reduce these risks while providing patients with definitive treatment options. More case studies such as this one, along with larger studies are needed to demonstrate the benefits of this technique for hepatic hydrothorax.
References
Doraiswamy V, Riar S, Shrestha P, Pi J, Alsumrain M, Bennet-Venner A, Kam J, Klukowicz A, Miller R. (2011). Hepatic hydrothorax without any evidence of ascites. ScientificWorldJournal. 2011 Mar 7;11:587-91. doi: 10.1100/tsw.2011.68 Case study.
Lee WJ, Kim HJ, Park JH, Park DI, Cho YK, Sohn CI, Jeon WK, Kim BI. (2011). Chemical pleurodesis for the management of refractory hepatic hydrothorax in patients with decompensated liver cirrhosis. Korean J Hepatol. 2011 Dec;17(4):292-8. doi: 0.3350/kjhep.2011.17.4.292. Eleven patient Korean study looking at the effectiveness of pleurodesis in patients with hepatic hydrothorax. While the procedure was successful in 8 patients, the authors noted a high rate of procedural-associated complications. (Notably, the researchers used several different agents for chemical pleurodesis.)
Sawant P, Vashishtha C, Nasa M. (2011). Management of cardiopulmonary complications of cirrhosis. Int J Hepatol. 2011;2011:280569. doi: 10.4061/2011/280569. Epub 2011 Jul 19. Article discussing complications of cirrhosis including hydrothorax.
Interested in learning more about single port thoracoscopy, or talking to the inventors of this technique? This March – head to the 1st Asian single port surgery conference in Hong Kong.
It doesn’t look like Cirugia de Torax will be in attendance for this conference, but it’s another opportunity for practicing thoracic surgeons and thoracic surgery fellows to learn more about single port thoracoscopic surgery.
This March (7th – 8th), the Chinese University of Hong Kong, along with the Minimally Invasive Thoracic Surgery Unit (Coruna, Spain), and Duke University are presenting the 1st Asian Single Port Symposium and Live Surgery conference in Hong Kong.
This is your chance to meet the experts – and the inventors of this technique (such as Dr. Diego Gonzalez – Rivas, one of the new masters frequently featured here at Cirugia de Torax.)
Dr. Chih-Hao Chen at Mackay Memorial Hospital in Taiwan talks about his experiences with single port/ single incision thoracic surgery (SITS) as well as the “Chen esophagectomy”; a new single port approach to esophagectomies.
Single-port thoracoscopic surgery (SITS) as a first-line approach
With the advent of minimally invasive surgical techniques such as VATS, surgeons now have the ability to perform multiple surgical procedures such as lobectomy, decortication and even esophagectomy through 1 – 2 cm port incisions instead of traditional open surgery. However, as mentioned during an interview with Dr. Mark Dylewski, few American* surgeons have fully embraced this technology. Even fewer surgeons internationally have embraced the emerging single port techniques that have developed from VATS. One of these surgeons is Dr. Chih-Hao Chen at Mackay Memorial Hospital in Taiwan. We previously discussed one of his studies here at Cirugia de Torax, so it was with great delight when we had an opportunity to discuss his continuing research and development in this area in a series of emails.
Dr. Chen is currently in the forefront of the movement to make SITS a first-line approach for majority of thoracic surgery procedures that can currently be approached with traditional VATS. The biggest risk to this “less is more” approach to port placement is needing to add additional ports during the case (thus converting to traditional VATS 3-4 port approach).
As Dr. Chen explains, “In contrast to creating 3 small wounds, I always try single-port first. If it is technically unavoidable, I would make the second port incision. If it is still difficult, a third port incision would be made. The conversion rate (to 2-port or three port methods not open) is very low in most conditions.
“I believe the role of SITS as a first-line endoscopic approach is possible in nearly all patients. So far, I have performed roughly, SITS in more than 150 patients with various thoracic diseases, including esophagectomy in 5 cases using 2.5 cm single incision”.
However, the contraindications for the SITS approach are mainly those with “unstable hemodynamics in trauma”, “highly complicated cancer resection(such as sleeve lobectomy, etc)” and “thick and dense peel in chronic empyema”.
Dr. Chen was kind of the provide this clip of him performing single port thoracoscopy.
Over 150 cases, so far.
“According to my experience, patients with spontaneous pneumothorax and acute stage empyema as well as solitary pulmonary nodules are the best candidates for such procedure. The time required for the same operation is much shorter in single-port approach. For simple spontaneous pneumothorax, the time may be as short as 20-25 minutes. ( from skin incision to suture )”.
As I mentioned in my report (see publications linked below), the conversion rate of such condition is pretty low and worthy to try. In my experience, SITS w/o trocar greatly decrease incisional pain and have pleasant cosmetic results, as the wound can be extremely small”.
A recent case: Wedge resection by SITS
Procedure: single-port approach for a case of lung cancer in a 77 year-old woman.
Multiple wedge resections, pleural biopsy and LN smapling were performed.
single incision (now with chest tube) and specimen removed (photo courtesy of Dr. Chen)
The wound was 1.5 cm in length and the specimen is 7cm X 4cm ( solid part :2.5 cm ). The specimen was removed within an endo-bag. (From previous experience, I knew that a specimen of this size can be safely removed through a tiny incision w/o destruction of the specimen.
Her chest tube was removed within 24 hrs and patient reports minimal discomfort. ( I injected Marcaine in ICS to prevent neuralgia in all cases.)
Sometimes innovation is hard
As we’ve seen frequently in the history of medicine / surgery, early innovators and adopters of new technology are often face significant resistance from their colleagues despite utilizing ‘best-evidence’ to support their ideas. People, many people, including surgeons – don’t like change and are sometimes hesitant to learn and practice techniques that develop in the years following fellowship.
One of the reasons Dr. Chen contacted Cirugia de Torax is to share his experiences and this technique with other interested thoracic surgeons. ‘Unfortunately, only a small portion of thoracic surgeons would like to try such procedure in Taiwan. Actually, most of them considered the procedure not valuable. Therefore, I would like to publish more experiences in the journals, which is one way to tell them “to try”.
Wait.. Did you say single-port thoracoscopy for esophagectomy?
“Esophagectomy in my team was performed by single-port thoracoscopic approach (in the chest). However, the abdominal portion was performed with four-port or 5-port laparoscopic approach, because the abdominal part was done by another doctor who is not familiar with single-incision laparoscopy (SILS). However, I have to admit that esophagectomy through single-port approach is much more difficult than other procedures. The main reason for this is that the esophagus is located in posterior mediastinum.”
While I usually utilize a more anterior ICS as my port incision for other single-incision procedures because the anterior ICS is very easy, with low conversion ( to 2- or 3-port ) rate. However, the same port is not appropriate for esophagectomy because of poor visualization.
New Approach, the “Chen esophagectomy” but ergonomic considerations
“For the reason, I tried a more lateral port incision (usually 5 ICS along the mid-axillary line. ) This is a BIG problem for me due to ergonomic issues. Manipulation of endoscopic instruments and the endoscope through the port is uncomfortable. At times, I have to rest for a while in order to alleviate soreness in my arm”.
“The time-determining step is to loop the esophagus. Proximal and distal dissection as well as lymph node dissection would be done with a harmonic scalpel. (We resected the esophagus, the anastomosis is in the neck ). For uncomplicated case, the procedure in the chest takes aroud 1-2.5 hours”.
*American research data suggests that VATS is used for less than 30% of all thoracic surgery procedures. However, anecdotal evidence suggests that internationally, VATS is utilized with much higher frequency outside of the United States.
Articles about single-incision thoracoscopic surgery (SITS) by Dr. Chih-Hao Chen
Checking in with Dr. Diego Gonzalez – Rivas and his team in Coruna, Spain – the innovators in single incision thoracic surgery, as Dr. Gonzalez publishes a new report on single incision pneumonectomy.
After speaking with Dr. Raimundo Santolaya last week – I contacted Dr. Diego Gonzalez over at UTCMI in Coruna, Spain to see what he’s been doing since our last contact, and discuss a possible interview in the future.
Last fall, he published another case report on single incision VATS – lobectomy, and since then he has continued to operate and publish reports on his successes. Now he has an upcoming case report on a right-sided single-port pneumonectomy, which was largely held as one of the last frontiers in VATS procedures. (Pneumonectomy by standard VATS, despite being reported in the literature several years ago, remains a relatively uncommon procedure.)
While a common criticism of his work is related to the fact that removing a portion of the lung as large as a lobe, or an entire lung requires a small additional incision at the conclusion of the case – but these criticisms are weak at best – and fail to see the true clinical importance of his continued innovation and investigation in advancing video-assisted thoracoscopic surgery for the benefits of our patients. Ten years from now – single incision VATS will be a common procedure, and Drs. Gonzalez, Fernandez and De la Torre will be the ones responsible.
References: Single port pneumonectomy
Gonzalez-Rivas D, de la Torre M, Fernandez R, Garcia J. (2012). Single-incision video-assisted thoracoscopic right pneumonectomy. Surg Endosc. 2012 Jan 11. [Epub ahead of print – abstract re-posted below]
Abstract
BACKGROUND:The most common approach for Video-assisted thoracoscopic (VATS) lobectomy is undertaken with three or four incisions, including a utility incision of about 3-5 cm. However, major pulmonary resections are amenable by using only a single utility incision. This video shows the technical procedure of a right pneumonectomy by single-incision approach with no rib spreading.
METHODS: A 52-year-old woman was proposed for single-incision VATS resection of a 5-cm right lower lobe adenocarcinoma. A 4-cm incision was made in the fifth intercostal space. We placed a 30-degree, high-definition, 10-mm thoracoscope in the posterior anterior part of the incision. Digital palpation confirmed that the tumor involved the fissure and the posterior portion of the upper lobe, which indicated the need for right pneumonectomy. We inserted the instruments through the anterior part of the utility incision to start the detachment of the right upper lobe by using a harmonic scalpel. The first step was dissecting the inferior pulmonary vein. The hilar structures were exposed by using harmonic scalpel and a long dissector (Fig. 1A). The upper and middle-lobe pulmonary veins were dissected and transected, allowing visualization of truncus anterior, which was then stapled. The inferior pulmonary vein and the intermediate truncus artery were divided, allowing optimal exposure to the main bronchus, which was stapled. The lung was removed in a protective bag by adding 1 cm to the incision, and a systematic lymph node dissection was performed. A single chest tube was placed in the posterior part of the utility incision.
RESULTS: Total surgery time was 210 min. The chest tube was removed on postoperative day 2, and the patient was discharged home on day 4 with no complications.
CONCLUSIONS: Single-port VATS pneumonectomy for selected cases is a feasible procedure, especially when performed from a center with previous experience in double-port VATS approach.
DISCUSSION:Recent advances in surgical and video-assisted techniques have allowed minimally invasive pneumonectomy to be undertaken safely. VATS pneumonectomy is not a new procedure and in fact was initially reported 15 years ago and was felt to result in less postoperative pain and a faster return to normal activities [1]. Despite this, there have been only a few case reports or series published of VATS pneumonectomies [2,3].
Additional References/ Resources
Gonzalez – Rivas, D., Fernandez, R., De la Torre, M., & Martin – Ucar, A. E. (2012). Thoracoscopic lobectomy through a single incision.Multimedia manual cardio-thoracic surgery, Volume 2012. This is an excellent article which gives a detailed description, and overview of the techniques used in single incision surgery. Contains illustrations, full color photos and videos of the procedure.
Gonzalez-Rivas D, Paradela M, Fieira E, Velasco C. (2012). Single-incision video-assisted thoracoscopic lobectomy: initial results. J Thorac Cardiovasc Surg. 2012 Mar;143(3):745-7.
Chen et. al discuss their experience with single incision thoracoscopic surgery (SITS) in the treatment of spontaneous pneumothorax in this Taiwanese study.
A study from Taiwan (April 2011) highlights the surgeons’ experience using single incision thoracoscopic surgery (SITS) for the treatment of spontaneous pneumothorax. While the study is small – involving 30 patients, with just ten patients receiving treatment via single incision thoracoscopy, it’s a useful study in demonstrating that SITS is not only possible but feasible for uncomplicated thoracic procedures.
The major advantage of using this procedure in the spontaneous pneumothorax population is the low level of underlying thoracic disease, or co-morbidities necessitating conversion to VATS or open surgery. In general, true spontaneous pneumothoraces occur in younger patients (teens and twenties) in the absence of other conditions such as infection, emphysema or effusion. The benefits of using this procedure in such a young, mobile population is reduced pain, and a speedier recovery – and returning these patients to work/ life faster, with less post-operative limitations.
As the authors noted, a consistent obstacle to widespread adoption of this surgical technique is the lack of specialized surgical instruments. This has also plagued single incision laparoscopy to some extent, with several minor modifications being made by practicing surgeons to overcome these problems, primarily of positioning several instruments thru a single port*. This is more problematic in thoracic surgery than general surgery due to patient positioning. (In general surgery the patient is usually laying supine, allowing for a flat surface).
Example of single incision laparoscopy for cholecystectomy
In thoracic surgery, the patient’s side lying positioning puts the operator at greater disadvantage, with gravity working against the surgeon. As mentioned in a previous post – there is a commercial port of multiple instruments available, however it is costly, unwieldly and requires larger incisions (making SITS more of a mini-thoracotomy). The other mechanical problem is the instruments themselves – when placed in a single incision, care has to be taken to prevent the instruments from obstructing the movements of each other. The authors were able to overcome this obstacle thru practice, but suggest needed modifications to existing instruments.
Despite frequently cited concerns about visibility with this technique, in the article (and confirmed by my own observations in the operating room), properly done single incision thoracoscopy offers the same visibility as multi-port (VATS) thoracoscopy. (See the original article full text for photos of procedure illustrating visibility.)
More recently, (June 2011) Berlanga & Gigirey in Caceres, Spain reported the use of SITS for spontaneous pneumothorax in 13 patients. They reported similar findings, and came to the same conclusions as Chen et. al. However, these researchers used the commercially available port and reported satisfactory results.
There is a place for single incision thoracoscopy within thoracic surgery. However, it will take continued research to further delineate its role, and surgical innovation to adapt the current instrumentation for more effective and surgeon friendly use.
Berlanga, L. A. & Gigirey, O. (2011). Uniportal video-assisted thoracic surgery for primary spontaneous pneumothorax using a single–incision laparoscopic surgery port: a feasible and safe procedure. Surg Endosc. 2011 Jun;25(6):2044-7. Epub 2010 Dec 7. Full text article not available for link (paid article).