In this post, we present a new video byTurkish thoracic surgeon, Dr.Cagatav Tezel on VATS decortication for tuberculosis.
There’s a new video over at VUmedi by Turkish thoracic surgeon, Dr. Cagatay Tezel. In this video, as well as a related article over at CTSnet, Dr. Tezel talks about modern day surgical treatment for tuberculosis related complications. Tuberculosis, unlike measles, polio or other diseases associated with the 19th (and earlier centuries) has not faded into the past, despite the availability of a (partially effective) tuberculosis vaccine. Tuberculosis continues to carry a heavy morbidity and mortality burden globally. In fact, for all of the news media surrounding Ebola, HIV, SARS and Bird/ swine and various flu, Tuberculosis is the real killer; and is responsible for 1.8 million deaths a year*.
Complicated multi-drug regimens and poor patient adherence have resulted in the development of new strains of resistant TB. Decreased immune resistance in specific populations such as diabetics, or patients with HIV infection has resulted in a greater number of people with active disease. This means, that thoracic surgery remains a critical component in the treatment of this deadly disease.
Surgical treatment of Tuberculosis and TB related complications
As long time readers know, Thoracics.org has been following the rise of multi-drug resistant (MDR-TB) and extreme/ extensive drug resistant (XDR-TB) versions of the age-old scourge of the ‘white plague‘ as well as the evolution of the surgical treatment of this disease, from the early era of thoracoplasty, as well as more modern treatment of TB related empyemas such as VATS.
In fact, the surgical treatment of tuberculosis is the foundation on which the thoracic surgery specialty emerged, out the operating theaters of TB sanitariums around the world. However, as the development and successful use of antibiotics spread from the late 40’s thru the 50’s and 60’s – surgery took a backseat to drug therapy. The development of these drug resistant strains means that it is imperative that the thoracic surgery community continue to research, innovate and operate on patients with tuberculosis.
We welcome articles and video submissions on this topic from our colleagues around the world.
*Several statistics give the annual death toll at 2 to 3 million.We have cited the most recent WHO figures above.
The Tuberculosis Vaccine: information about the vaccine, and who should get it (according to current CDC recommendations).
Freixinet JG1, Rivas JJ, Rodríguez De Castro F, Caminero JA, Rodriguez P, Serra M, de la Torre M, Santana N, Canalis E. (2002). Role of surgery in pulmonary tuberculosis. Med Sci Monit. 2002 Dec;8(12):CR782-6.
Case report with video of SITS (single incision thoracoscopic surgery) repair of diaphragm defect in a case of hepatic hydrothorax resulting from liver cirrhosis with Dr. Chih-Hao Chen, MAckay Memorial Hospital, Taiwan
Case Report: Single incision thoracoscopic repair of diaphragmatic defect in a patient with hepatic hydrothorax
Dr. Chih-Hao Chen, Thoracic Surgeon MAckay Memorial Hospital, Taiwan
Dr. Chen, Thoracic Surgeon
Clinical History:
Patient is an elderly woman who was admitted after a motor-vehicle accident with a traumatic fracture of the humerus and femoral neck. She was brought to our ED immediately and was intubated due to acute respiratory failure.
Subsequent Chest radiograph showed diffuse opacity in right hemithorax and concomitant fracture in left side humerus and femoral neck. Attempt for tapping of the pleural effusion showed clear in nature.
According to previous medical records, she had no relevant history. She was admitted to ICU for further evaluation and management.
Fluid analysis in emergency department showed transudate.
LFTS: Total Bilirubin 2.7 mg/dL AST 116 ALT 68 Albumin 2.3 g/dL Direct Bilirubin H 1.1 mg/dL
Chem panel: BUN 83 mg/dL Creatinine 1.6 mg/dL K 3.2 mEq/LNa 144 mEq/L
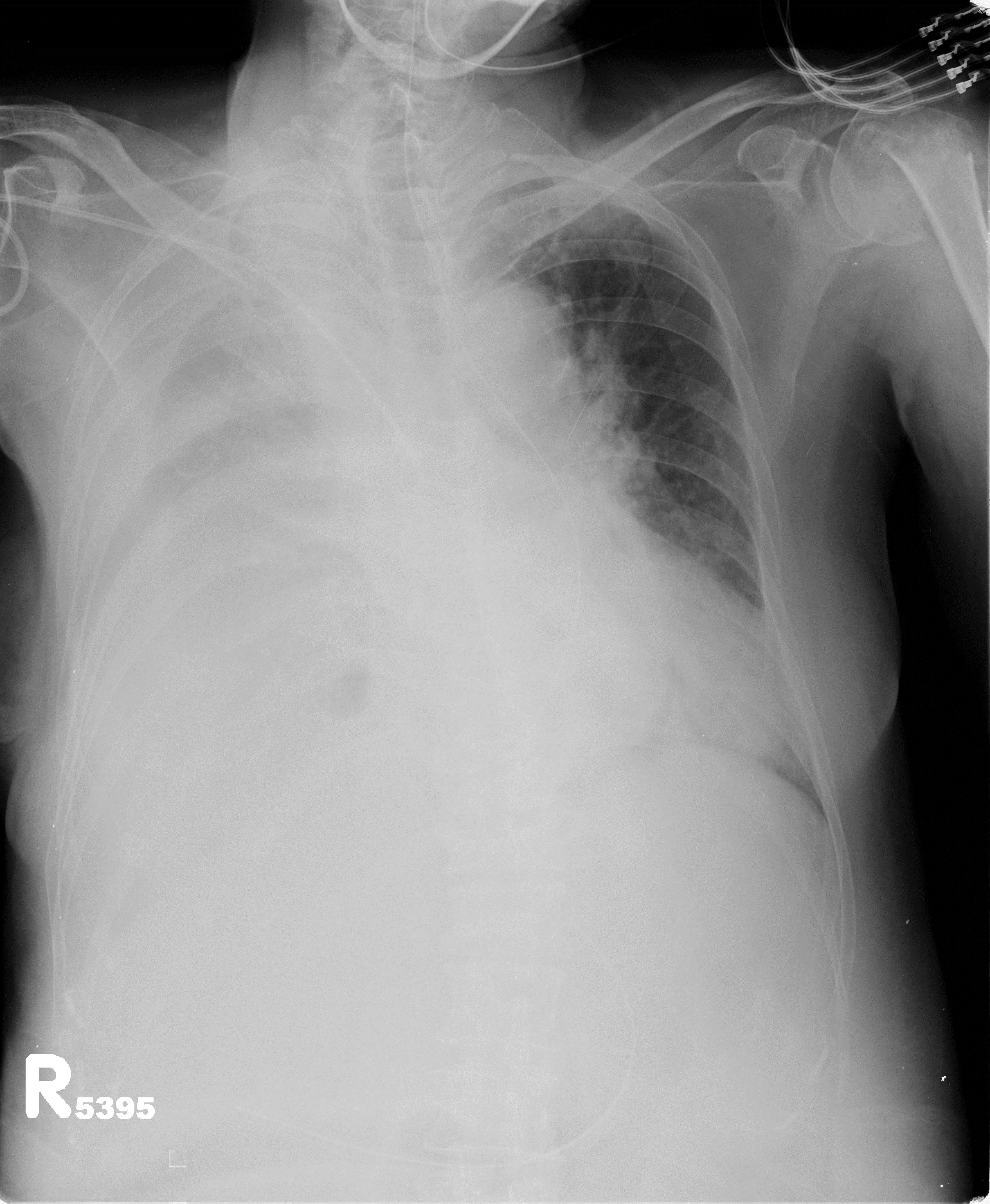
Chest radiograph on admission showed a massive right-sided pleural effusion.
Chest radiograph on admission
For symptomatic control, the physician performed intermittent thoracentesis. Because the traumatic site is left aspect of the trunk ( fracture in left side humerus and left side femoral neck ) and right side effusion was very clear.
Hepatic hydrothorax was suspected. Later peritoneal scan confirmed the diagnosis.
Peritoneal scan
The scan showed left side pleural space was sparring from radioisotope. Direct communication between right side pleural cavity and the abdomen. The diagnosis is confirmed with such findings.
CT scans are not diagnostic for this condition, and were not indicated for her other injuries. Therefore, we did not arrange CT scan of the chest / abdomen.
Abdominal ultrasound showed moderate to massive ascites. Along with hepatic encephalopathy, moderate to massive ascites, prolonged PT/PTT, low albumin, higher bilirubin, the extent of cirrhosis is Child’s class C.
Operative Procedure: Single incision thoracoscopic repair of a diaphragmatic defect. Theoretically, with SITS, the wound can be very tiny. However, in our experience (fifteen total cases to date), diaphragm surgery through single port may be a bit difficult because we did not know where the defect is. We have to inspect very carefully and to search for the defect where the fluid came out. In this case, we made one small wound around 2 cm in length at the 6th ICS along the anterior axillary line.
Repair of the diaphragmatic defect was performed using silk suture similar to that used to repair inguinal hernias. Intra-operatively, the defect was 2 -3 mm in diameter.
At the conclusion of the procedure, using the original incision, we placed one Fr.24 chest tube to monitor the drainage and may consider chemical pleurodesis if the drainage persists. The operative procedure was accomplished within 30 minutes.
Post-operative Chest Radiograph
Post-operative condition of the chest film showed near complete resolution of the effusion and lung re-expansion was complete.
Pathology/ Fluid Cytology: fluid analysis and peritoneal scan showed communication between peritoneal space and right side pleural space confirming pre-operative diagnosis. No tissue specimens were taken during this procedure.
Discussion:
Hepatic hydrothorax is the development of a pleural effusion in a patient with liver disease in the absence of cardiopulmonary pathology, making it a diagnosis of exclusion in many cases. It can occur in patients with and without ascites and may be the first presenting symptom in patients with undiagnosed liver disease. Similar to catamenial pneumothorax; hepatic hydrothorax is predominantly a right-sided disease. This is due to an anatomic gutter or diaphragmatic defect that occurs, and allows the passage of material or fluid from the abdominal cavity into the pleural space. This can be seen and identified on peritoneal studies(Peritoneal scan) like the study showed in our case study above. (Similar pathologies can occur in related conditions such as renal failure related hydrothorax due to this defect). Such defect is usually identified in the tendon part of the diaphragm. Peritoneal scan can confirm there is communication between the abdominal cavity and the pleural space. However, the definite location, size and number of defects can not been identified by the scan alone. Thoracoscopic inspection is the only method to search for such defect(s).
Video-assisted thoracoscopic surgery (VATS) has been shown to be a safe and effective method of treating this condition, by allowing surgeons to correct the defect, and thus prevent recurrence (Saito et al. 2012). The cure rate varied greatly in the literature. The key is whether the defect can be repaired. For one to two obvious defects, direct suture repair usually cured the disease. (the cure rate more than 80%) However, for some undetectable defects or defects with fenestration type, the cure rate is very low, ( around 30-50% ). Alternative strategies have to be considered in such condition, such as tissue glue, abrasion pleurodesis, mesh interposition and using sclerosing agents(OK432, bleomycin, Minocin, talc, etc). This is in distinct contrast to the numerous non-surgical drainage procedures such as thoracentesis, which removes accumulated fluid but does not correct the underlying pathology. However, the hallmark of this condition, liver failure predisposes patients to complications such as bleeding, infection and poor wound healing. These risks are one of the primary reasons treatment was often limited to drainage procedures prior to the popularization of lower risk VATS procedures. In the past, patients with Child’s class C liver cirrhosis are basically not proper surgical candidates because of extremely high mortality/morbidity rate. In recent experience of single-port approach, some patients with Child B and C are still safe with minimal postoperative complications. The advance of these minimally invasive technologies such as uni-port thoracoscopy permits fewer and more limited incisions which is believed to further reduce these risks while providing patients with definitive treatment options. More case studies such as this one, along with larger studies are needed to demonstrate the benefits of this technique for hepatic hydrothorax.
References
Doraiswamy V, Riar S, Shrestha P, Pi J, Alsumrain M, Bennet-Venner A, Kam J, Klukowicz A, Miller R. (2011). Hepatic hydrothorax without any evidence of ascites. ScientificWorldJournal. 2011 Mar 7;11:587-91. doi: 10.1100/tsw.2011.68 Case study.
Lee WJ, Kim HJ, Park JH, Park DI, Cho YK, Sohn CI, Jeon WK, Kim BI. (2011). Chemical pleurodesis for the management of refractory hepatic hydrothorax in patients with decompensated liver cirrhosis. Korean J Hepatol. 2011 Dec;17(4):292-8. doi: 0.3350/kjhep.2011.17.4.292. Eleven patient Korean study looking at the effectiveness of pleurodesis in patients with hepatic hydrothorax. While the procedure was successful in 8 patients, the authors noted a high rate of procedural-associated complications. (Notably, the researchers used several different agents for chemical pleurodesis.)
Sawant P, Vashishtha C, Nasa M. (2011). Management of cardiopulmonary complications of cirrhosis. Int J Hepatol. 2011;2011:280569. doi: 10.4061/2011/280569. Epub 2011 Jul 19. Article discussing complications of cirrhosis including hydrothorax.