Thoracics.org is here with registration information for two upcoming thoracic surgery conferences online.
With the continuing pandemic, and related infection control measures, the majority of thoracic surgery conferences have been postponed or cancelled. However, the are two upcoming online thoracic surgery conferences to take note of.
This webinar hosted by the Argentine Society of Thoracic Surgeons, and Dr. Hector Rivero. Interested readers may register for this webinar at this link: Register for Webinar 26 June 2020.
Duke Masters of Minimally Invasive Thoracic Surgery
While readers have just a few days to register for the conference above, there is considerably more time to register for the 13th Annual Masters of Minimally Invasive Thoracic Surgery – Virtual Conference. While the traditional conference has become the annual pilgrimage south – this year’s online offering offers opportunities for greater attendance and participation from surgeons outside North America.
This conference runs September 25th, 2020. Interested readers may click here to register. The full online schedule of speakers has not yet been published
There were plenty of reasons for surgeons from all over Latin America to converge on Cuscu, Peru for the 2nd annual VATS PERU Uniportal Master Class, which covered the basics of the uniportal approach as well as nonintubated and awake uniportal surgery. There were subxiphoid and uniportal cases streamed live from Shanghai Pulmonary Hospital. But beyond the usual reasons of networking, discussing and sharing case knowledge, and the presentation of research findings and evidenced-based practice, there were several reasons why VATS Peru was more than just your average regional thoracic surgery conference.
Why attend VATS Peru? The three best reasons:
1. The wet lab – which allowed surgeons and their surgical assistants to apply the theoretical knowledge they learned during the first two days of lecture in operating room scenario en vivo. The “en vivo” is critical, fancy simulators aside, there is no better challenge to ‘book knowledge’, and application of practical skills than in the scenario of an operating room, with real models and active bleeding.
A surgeon in the master course receives instruction from Dr. Diego Gonzalez Rivas
2. Lectures from the master surgeon himself; Dr. Diego Gonzalez Rivas: That’s where the second critical component comes in, in the form of the candid, direct and straight-forward lecture by Dr. Diego Gonzalez Rivas on Control of Inter-operative Bleeding. If you weren’t paying attention during this lecture, it’s obvious in the lab. This isn’t a computer course where you can dial in your answers, fast-forward thru lectures and print off a shiny new certificate. This isn’t a computer app, or a simulation that you can reset and re-start as soon as the surgery heads off course, to try again.. It’s real surgery.
3. Dr. Carlos Fernandez Crisosto
Lastly, if you didn’t attend VATS Peru, then you missed an opportunity to know and to talk to Dr. Carlos Fernandez Crisosto. VATS Peru is his brainchild, and the organization was created specifically to advance minimally invasive surgery in Peru. VATS Peru is separate from ALAT (the Latin American Society of Thoracic Surgeons), of which Dr. Fernandez is the current president. VATS Peru is also separate from the Peruvian Society of Thoracic Surgeons which has its own focus in the thoracic surgery specialty.
Dr. Carlos Fernandez Crisost0, Cardiothoracic and Vascular surgeon
Dr. Fernandez, a Tacna native, works at Daniel Alcides Carrion Essalud facility in the southernmost region of Peru. He is the sole cardiovascular and thoracic surgeon for the city of Tacna, and performs cardiac, vascular, and endovascular surgeries in addition to general thoracic surgery. While he is a trained cardiovascular surgeon, (in addition to general thoracic) thoracic surgery is what he enjoys most.
He trained in Argentina, and practiced in Cordoba, Argentina for 23 years before returning to Tacna in the last few years.
His average case volume is around 380 surgeries a year, and he reports that all of his thoracic surgeries are generally performed using the uniportal thoracoscopic approach. He also does transplant, which requires him to travel to Lima specifically to perform the procedure. The transplant program is small and performs 4 to 5 transplants per year.
In his practice he sees the usual oncology cases, and empyemas but he also sees a large number of patients with tuberculosis, as well as an assortment of hydatid cysts, and pectus cases. Trauma from accidents, as well as injuries from guns, and knives also comprises a large part of his practice.
Dr. Fernandez is pleased with the success of his course, since this is only the second time the course has been available here in Peru. It was a complex logistical arrangement to hold the course in Cusco this year, but with the help of his wife, a professional events planner, they were able to pull of the event with very few hiccups. Next year, they plan to hold the event in Lima, the capitol of Peru and a city famed for its gastronomic offerings.
If you missed this year’s VATS Peru, look for VATS Peru 2017 here at Thoracics.org next fall.
Single port thoracoscopic surgery and awake anesthesia: the micro-invasive thoracic surgery? The current research and use of these state of the art techniques to bring minimally invasive surgery to complex surgery and high risk patients.
At a recent high-profile American thoracic surgery conference, one of the speakers presented data from his program showing the safe and effective use of regional and conscious sedation techniques to perform complex thoracic surgery procedures on non-intubated patients.
Instead of being greeted with enthusiasm or professional interest, the great majority of well-known giants in thoracic surgery dismissed the idea with a few, repeated sarcastic, albeit joking remarks about the inconvenience of having conscious patients in the operating room. This attitude seemed perplexing given the results of Pompeo et; al.’s (2014) survey of the European Society of Thoracic Surgeons, in which a large number of respondents (59%) reported using nonintubated thoracic surgery (NITS) procedures. These mixed attitudes led thoracics.org to perform an in-depth literature search to determine the state of non-intubated thoracic surgery.
What is the current status of non-intubated thoracic surgery (and the literature surrounding it)?
Is it a wild, unsustainable idea promoted by a few dynamic but misguided surgeons? Is it a well-researched and promising developing technique that is being rejected by surgeons who may lack vision? Or does it fall into that gray area where we suspect that this technique has real value and benefits for a special subset of patients but there isn’t quite enough high level clinical evidence to demonstrate that to the surgical community?
Is non-intubated thoracic surgery destined to fall to the same fate of VATS – a game-changing technique that emerged in the early 1990’s, has been clinically demonstrated to be superior to open surgery with an overwhelming preponderance of evidence, but still being discussed by many surgeons as the ‘new kid on the block’**? Will people still debate the merits of non-intubated surgery ad infinitude thirty years from now, even when clinical guidelines have made it the standard of care (like VATS and oncology surgery)? Will there be the same reluctance to set firm standards for training in these techniques?
“Not a new concept”
photo courtesy of the US Army
As it turns out – non-intubated thoracic surgery is not a new idea or concept. It was developed early in the 20th century and was used successfully for many years for even the most complex thoracic cases such as esophagectomies until the development of double lumen intubation in the 1950’s made the use of single lung ventilation possible (Gonzalez-Rivas et. al. 2015, Pompeo 2015, Kiss & Castillo 2015). Since its rediscovery in the last several years, many of the problems that plagued this technique during its inception over a century ago have been addressed through better understanding of human physiology. Now, this seemingly fringe technique has been shown to be a feasible approach for treating the very margins of the thoracic surgery population (the extreme elderly, patients with advanced respiratory disease or other serious medical co-morbidities) that are often deemed inoperable using current techniques.
The dreaded complication (spontaneous pneumothorax) of early use of this technique by pioneers in thoracic surgery has now become one of the main advantages. Surgically created pneumothorax results in almost perfect deflation of the operative lung, achieving better results than even the most experienced of anesthesiologists using traditional single lung ventilation. Surprisingly to many observers, instead of creating a ventilatory emergency, this process is readily tolerated by most patients, even those with poor baseline pulmonary function (David, Pompeo, Fabbi & Dauri, 2015).
Current research
The majority of the current series of research on this topic are being performed by a small group of surgeons which includes Dr. Diego Gonzalez Rivas (Spain), Dr. Eugenio Pompeo and the Awake Thoracic Surgery Research Group in Italy and Dr. Ming-Hui Hung and colleagues (Taiwan). Pompeo’s group (Drs Benedetto Cristino, Augusto Orlandi, Umberto Tarantino, Tiziana Frittelli (General Director of the Policlinico Tor Vergata), Leonardo Palombi, Paola Rogliani, Roberto Massa, Mario Dauri) has been especially prolific in 2015 after several of their works were published in a special issue of Annals of Translational Medicine.
In multiple studies, these researchers have reported successful thoracic surgery outcomes in non-intubated patients, thus eliminating the majority of risks related to general anesthesia as well as uni-lung ventilation via mechanical ventilation and intubation. In several of these studies, the authors were also able to successfully perform these surgeries in fully awake patients (versus consciously sedated), making surgery possible for even the frailest of candidates. These studies included a small number of comparisons between traditional and non-intubated surgeries. While the numbers of patients enrolled have been small, and there are few randomized studies, the results have been encouraging.
Chen et. al
Chen et. al’s 2012 study has been one of the largest studies to date, with 285 cases. In this study, patients underwent lobectomies, wedge resections and segmentectomies with 4.9% requiring conversion with tracheal intubation. Lung resection was undertaken with traditional (3 port) VATS or a needlescopic approach.
The authors report the biggest problem they encountered was increased bronchial tone and airway hyper-reactivity during manipulation of the pulmonary hilum during lobectomies and segmentectomies. This was effectively treated without significant alteration in hemodynamics via intrathoracic vagal blockage which eliminated the cough reflex in these patients.
The authors caution judicious patient selection to prevent emergent conversion (intubation) particularly while surgeons are initially attempting this technique. Chen et al. also believe that non-intubated thoracic surgery is best suited for petite or small-sized female patients because the small tracheal size of these patients predisposes them to a higher rate of complications and potential tracheal injury with traditional surgery and intubation.
Awake anesthesia and lung volume reduction surgery
Pompeo et. al’s review of the literature surrounding of the use of this technique in patients with severe emphysema undergoing nonresectional lung volume reduction surgery (LVRS by awake anesthesia) showed significant treatment advantages for patients undergoing lung volume reduction surgery without intubation or administration of general anesthesia.
With an average mortality of 5% and a morbidity of 59% for traditional lung volume reduction surgery as reported during the National Emphysema Treatment Trial, findings from Tacconi et al.’s 2009 study of 66 LVRS awake patients (matched with 66 patients undergoing traditional surgery) appears promising. The authors report a reduced incidence of prolonged air leaks (18%) versus 40% in the traditional surgical group as well as a decreased length of stay. In this study, 3 patients required conversion to general anesthesia – one patient due to an elevated paCo2 of 83% and the remaining two patients for anxiety attacks.
Rate of intubation/ respiratory failure/ mortality in Tacconi et al.
Mortality in both non-intubated and the traditional surgical group was the same, with one patient from each group. In both cases, the patients had developed massive airleaks following surgery. In the non-intubated group, the patient developed acute lung injury requiring intubation of POD#12 and died POD#38.
In the traditional surgical group, 4 patients were unable to be extubated at the end of the case, with one patient requiring an additional day of mechanical ventilation. Another patient was reintubated on POD#3 for respiratory failure and died on POD#67.
Pompeo et. al, over the course of over eleven years, have also investigated the use of non-intubated (and awake) thoracic surgery for a wide variety of cases including urgent /emergent cases, wedge resections, decortications, talc pleurodesis as well as nonintubated anesthesia combined with single (uniportal) thoracoscopic approaches (aka “microinvasive thoracic surgery”).
Anesthesia for non-intubated thoracic surgery
The role of anesthesiologists in caring for patients undergoing non-intubated or awake thoracic surgery is more challenging than general anesthesia. While thoracic anesthesia already requires specialized skills for initiating, managing and maintaining uni-lung ventilation, the switch to non-intubated patients with either localized anesthesia or conscious sedation adds a new set of complexity to managing these often frail patients. Kiss & Castillo (2015) in their review of the literature, provide an excellent overview of the pros and cons of non-intubated anesthesia as well as guidelines for patient selection and eligibility criteria for use of this technique. Special populations who may benefit from this technique include patients with severe respiratory disease (and a high risk of ventilator dependency with intubation), patients with severe but stable dyspnea, or multiple cardiovascular and respiratory co-morbidities.
Kiss et. al also reviews the contraindications to use of this technique including: phrenic nerve paralysis on the non-operative side, patients at risk for difficult intubation, or patients who are unwilling to undergo awake thoracic surgery. Wang & Ge (2014) expand on these complications to include ASA status 4 or higher, bleeding disorders, decompensated heart failure, extreme obesity, unfavorable airway or spinal anatomy as well as specific respiratory conditions including bronchiestasis, asthma, sleep apnea, clinically significant sputum production and strict contralateral lung isolation.
Wang & Ge also give specific anesthesia dosing guidelines for conscious sedation, local anesthesia and regional blocks in additional to monitoring parameters.
Alterations in oxygenation and ventilation
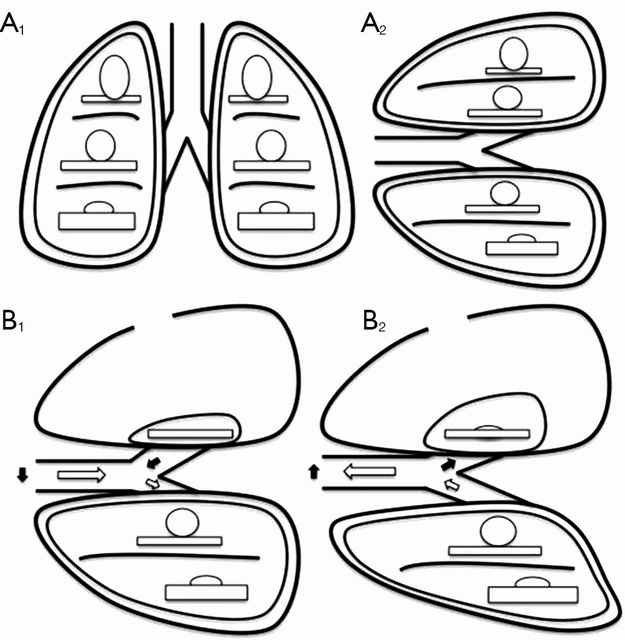
David et. al. (2015) describe the pathophysiology and alterations in oxygenation and ventilation in surgical pneumothorax including hypercapnia, hypoxia and the associated hypoxic pulmonary vasoconstriction that occurs along with the development of intrapulmonary shunt as the deflated (and unventilated lung) maintains perfusion. The authors also explain how this effect can be either exacerbated or minimized thru the choice of anesthetic agents, and the administration of supplemental oxygen, which further demonstrates the importance of involving the thoracic anesthesia team in preparation for non-intubated cases.
The relationship between ventilation and perfusion. (A) Relationship between ventilation (roundes) and perfusion (rectangles) in different lung zones, in upright (A1) and lateral position (A2); (B) relationship between ventilation (roundes) and perfusion (rectangles) in lateral position with surgical pneumothorax, during spontaneous inspiration (B1) and exhalation phase (B2). Black arrows show paradoxical ventilation and mediastinal shift. (Illustration and caption from David et. al, 2015)
This “permissive hypercapnia” has been reported in multiple articles as having minimal to no clinical effects and is easily treated with supplemental oxygen by nasal cannula or facemask.
Editor’s note: In advance of this article, Dr. Pompeo, Dr. Gonzalez Rivas and Dr. Min-Hui Hung were contacted for their additional comments and insights on non-intubated thoracic surgery. This and subsequent articles may be augmented, as applicable with their replies.
Conclusion
Should we really abandon pursuit of better patient outcomes, faster mobility, recovery and reduced length of stay in lieu of the security to tell off-color jokes with our patients safely under general anesthesia? Should we abandon all hope in treating patients previously deemed inoperable due to our own fears and hesitations to embrace newer techniques and procedures?
Or as Mineo et al, suggests, should we enlist our colleagues to design and devise several large scale studies at multiple institutions so that we can move to the next level of investigation and answer the question: “Should my patient be awake for this?”
Mineo TC, Tacconi F. (2014). Nonintubatedthoracic surgery: a lead role or just a walk on part?Chin J Cancer Res. 2014 Oct;26(5):507-10. doi: 10.3978/j.issn.1000-9604.2014.08.11. No abstract available. Very enjoyable, almost conversational article with the authors sharing their experiences with non-intubated thoracic surgery while calling for larger clinical research studies on the topic.
Pompeo, E. (2015). Non-intubated thoracic surgery: nostalgic or reasonable? Annals of Translational Medicine, 2015; 3(8): 99. Review of the historical development on non-intubated thoracic surgery and techniques in regional anesthesia for complicated thoracic surgery procedures including esophagectomies in the era predating the development of double lumen intubated and unilung ventilation. A timely reminder that some of the greatest developments in medicine and surgery are ‘rediscoveries’ of our predecessors.
Pompeo E; Awake Thoracic Surgery Research Group (2012). To be awake, or not to be awake, that is the question. J Thorac Cardiovasc Surg. 2012 Jul;144(1):281-2; author reply 282. doi: 10.1016/j.jtcvs.2012.01.083. No abstract available. Comment on article by Noda et. al.
Note: This is not an exhaustive list of literature available on this topic but a select listing of the most recent and relevant citations (and are available as free full text).
**Long time readers of thoracics.org may have noticed that we no long cover or report on ‘debates’ or discussions as to whether VATS can be used in oncology cases, or whether an adequate lymph node dissection can be performed using VATS. The literature clearly demonstrates that it can – and clinical guidelines reflect this, making the discussion one-sided, tedious, out-dated and repetitious.
Dr. Diego Gonzalez Rivas discusses intubated and nonintubated uniportal thoracic surgery for complex thoracic procedures
Orlando, Florida
Dr. Diego Gonzalez Rivas discusses non-intubated thoracic surgery
One of the standout presentations on Day One of the Duke Masters of Minimally Invasive Thoracic Surgery was Dr. Diego Gonzalez Rivas’ presentation on performing uniportal surgery on non-intubated patients. Surprisingly, this presentation was greeted with significant skepticism in the form of comments by fellow presenters.
No trocars, no rib spreading, one incision (with no rigid port placement)
The use of one small 2.5 cm incision with the camera placed above the instruments allows the surgeon to maintain the traditional perspective of open surgery using a minimally invasive approach. “Eyes above hands” Dr. Gonzalez states, reminding surgeons how to keep their visual perspective unaltered. He also discussed some of the findings from an upcoming 2016 paper [in-press] entitled, “Pushing the envelope” which reviews the developments in the areas of single port (uniportal) thoracic surgery in non-intubated patients. This along with his new textbook, have dominated the international thoracic surgery news in recent years.
As part of his discussion, he demonstrated the ease and feasibility of performing a complete and thorough lymph node dissection using the uniportal approach.
Complete paratracheal lymph node dissection in a non-intubated patient
He also presented several complex thoracic cases such as a bronchial sleeve resection for carcinoid tumor in a young, otherwise healthy female, as well as a double sleeve case, and a uniportal bronchovascular reconstruction. He discussed distal tracheal resection using high frequency ventilation jet in a non-intubated patient after resecting the carina – tracheal anastamosis and several chest wall resection cases via the uniportal approach. But the main portion of his talk was devoted to the specifics of non-intubated surgery – from anesthesia protocols to creating a anatomic (surgical) pneumothorax which eliminates problems of lung inflation during surgery. He discussed that while totally awake nonintubated surgery can be performed (with patients awake and talking), that he prefers the use of conscious sedation for patient comfort.
Nonintubated patient – VATS lobectomy
He highlighted the benefits of these approaches – with non-intubated surgical techniques allowing surgeons to operate on frailer, sicker patients who might otherwise be ineligible for surgery. He also talked about the benefits of uniportal surgery versus robotic surgery. Uniportal surgery is faster, and cheaper than costly robotic techniques that require lengthy patient positioning as well as the use of robotic tools that have to be replaced after 10 to 20 cases.
He also reviewed the relative contraindications for nonintubated surgery:
obese patients (BMI greater than 35)
patients with Malpati scores of 3 or 4 (difficult to intubate patients – in case of the need for emergent intubation)
patients with pulmonary hypertension (who will not tolerate permissive hypercapnia)
Masses greater than 6 cm in size
But he also reminded attendees that relative contraindications often change in the face of more experience.
Dr. Diego Gonzalez Rivas headlines the ALAT sponsored event this September.
Cardiothoracic surgeon and the coordinator and director of VATS Peru, Dr. Carlos Fernandez Crisosto cordially extends an invitation for all interested thoracic surgeons to attend VATS Peru. This event is co-sponsored by ALAT being held at the Hospital Essalud Tacna in Tacna, Peru on the 21st and 22 of September. The 2 day course includes a wet-lab for a hands on approach at teaching uniportal VATS with Dr Gonzalez Rivas.
Thoracics.org has written for additional information – so I will update this post as information arrives. To register – click here.
Corrections: as many readers know, I do much of my writing on the fly, in airports, waiting rooms etc. The sometimes results in spelling and grammatical errors. As always my sincere apologies.
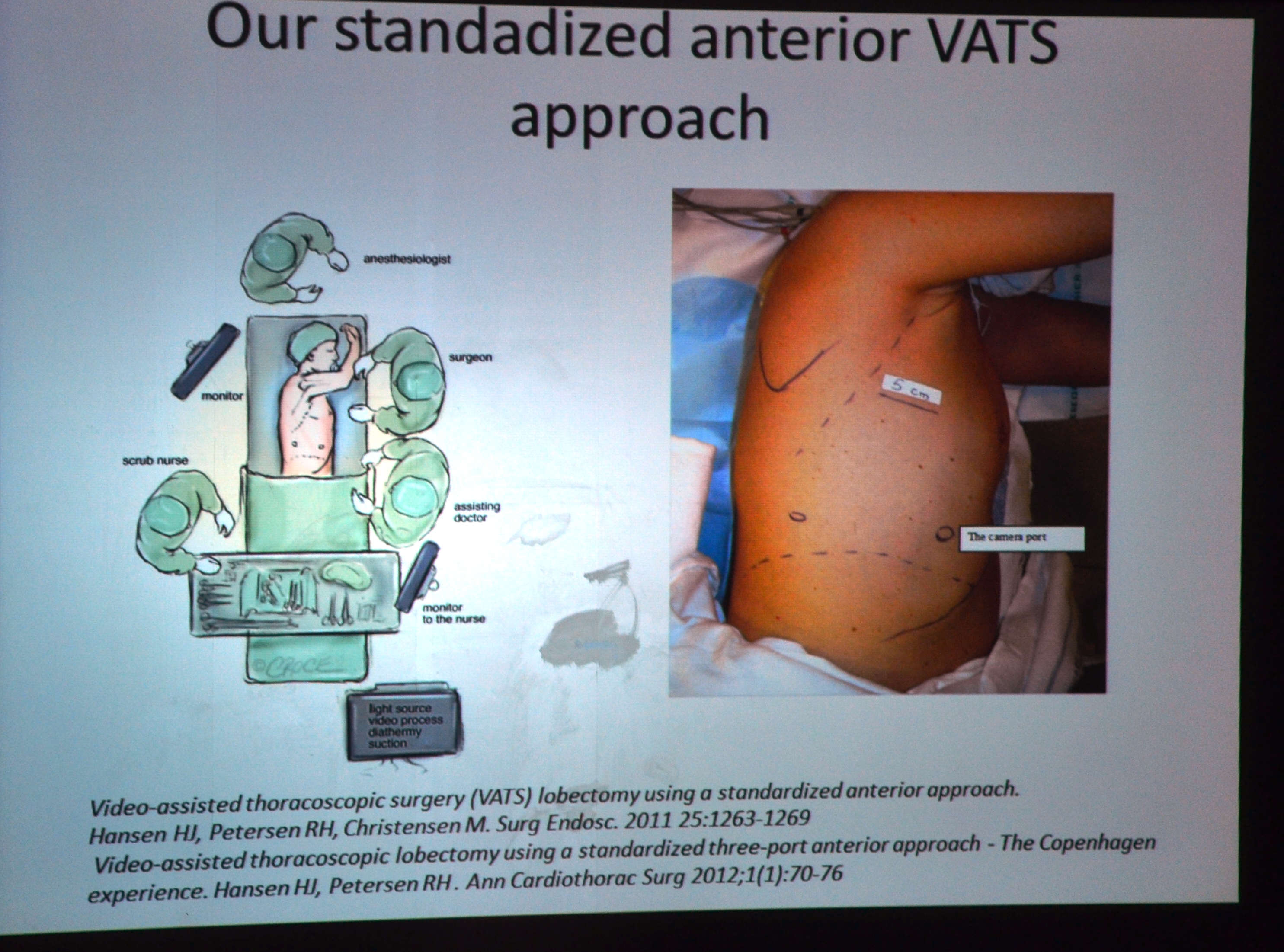
Dr. Henrik Hansen on how to streamline your surgery, and Dr. Diego Gonzalez Rivas at the Live surgery sessions of the Minimally invasive surgery conference in Naples, Italy.
Monaldi Hospital – If these walls could talk
Hospital Monaldi
It’s the second day of the conference at Monaldi Hospital which is located in Zona Ospedale, in the hills of Naples. The corridors of the 800 bed, 135 year-old former tuberculosis sanitarium give away few hints of the rich and interesting history of this institution. Commandeered by the Allies during the second world war, and containing a small but extensive pathology museum hidden in a back office, showcasing lung disease and many of the disseminated tuberculosis cases that were cared for here, one can only be intrigued by the stories contained within such as the first specimen in the collection, a five month’s gestational fetus (in utero) of a deceased tuberculosis patient.
Dr. Majorino, thoracic surgeon (who has worked at Monaldi Hospital for over 30 years and the head of the pathology department – in the museum of pathology
But we digress. As intriguing as all the tales of thoracic disease past are, we are gathered here today to advance the present and change the future of thoracic surgery here at Monaldi Hospital. As mentioned in a previous post, the surgeons here in the department of thoracic surgery have only recently adopted VATS surgery. Now after four years of practice, it is time to perfect it. For that reason, the first guest surgeon to perform the live demonstration today is Dr. Henrik Hansen.
Live Surgery with Drs. Hansen & Gonzalez Rivas
Dr. Henrik Hansen
Dr. Henrik Hansen
Dr. Hansen is a Denmark native who currently operates in one of Europe’s busiest VATS programs, located in Copenhagen. 80% of all the thoracic surgeries performed at his institution, Rigshospitalet. (In comparison, in most of Europe, VATS comprises of 52% of thoracic procedures, according to data presented by Dr. Hansen).
As the head of the minimally invasive surgery department at Righospitalet, he has mastered and streamlined the ‘traditional’ or three-port VATS approach, so there are no wasted efforts to maximize efficiency.
During a short lecture prior to surgery, Dr. Hansen discussed the literature, including a paper by WS Walker et al. in 2003, which compared cancer survival outcomes in patients undergoing VATS and standard open procedures. In the paper, the authors unequivocally recommended VATS as the operation of choice. It was this paper that led Dr. Hansen to aggressively pursue VATS for the majority of his patients. This position was not echoed in the official guidelines until 2013.
slide from Dr. Hansen’s presentation
Dr. Hansen allows that not all cases should be VATS cases; he prefers to perform sleeve resections via thoracotomies instead of VATS pneumonectomies, to prevent excess tissue loss in these cases).
Interestingly enough, residents in Dr. Hansen’s program learn VATS techniques without knowing the equivalent open surgical technique. He cites one of his thoracic surgery fellows as performing over 80 VATS procedures but only two thoracotomies. As a surgery purist, this disturbs me in some way, but then again – by much of Dr. Hansen’s criteria, I would be labeled a traditionalist.
For the morning’s case, he is performing a left upper lobectomy. (There are no other case details available to spectators in the auditorium)*.
He places the first port along the transverse line where the standard thoracotomy incision would normally be placed. He then triangulates the second and third ports, though only one actual trocar port is used, a 12 mm port for the camera insertion.
The “working” incision is the uppermost incision, which appears to be quite large, (but this may be a distortion due to my perspective – from a camera placed above the operating room table). At times he uses more than one instrument in this incision – and watching him, he seems that he could easily convert to single port surgery with equal efficiency. He almost forgets about his second port at times, and uses the remainder (3rd port) solely for the camera access.
He is precise and exacting in his movements, which is what makes his reliance on traditional VATS a little puzzling. Habit, mainly, I suspect because the surgery proceeds as if by rote. He really is the master of efficiency – and the case progresses quickly.
He uses ligasure for greater precision during dissection and isolation of tissue and minimizes the external torsion and retraction placed on the lung during hilar dissection, isolation and ligation of the pulmonary vasculature. He completes the procedure by performing an extensive lymph node dissection.
*Since I was outside of the operating room for this case, there are not very many operative photos, and none of Dr. Hansen operating.
Dr. Diego Gonzalez Rivas
As part of his pre-surgical lecture, “Recent advances in uniportal VATs,” Dr. Gonzalez reviewed the recent history of uniportal VATS as well as surgical tips for surgeons learning the technique. He also reviewed some of his more recent forays into surgery including complete uniportal resections using only the harmonic scalpel, and surgery on non-intubated (and awake) patients on nasal cannula. He discussed that the non-intubated project was a anesthesia counterpart to minimally invasive surgery. Since the risks and complications related to thoracotomies and other large incisions have been eliminated, it’s a normal progress to advance towards less invasive anesthetic techniques (since general anesthesia is associated with serious risks such as severe hypotension, peri-operative myocardial infarction and cardiovascular collapse). While rare, eliminating general anesthesia in many cases, greatly reduces the risk of adverse anesthesia-related events.
Surgical procedure**: Left upper lobectomy with radial lymph node dissection for a left upper lobe peripheral nodule in a 65 year patient.
Pre-operative CT scan
Surgeon: D. Gonzalez Rivas. Assistant Surgeon: D. Amore Scrub nurse: Guiseppe
1445: Initiation of patient prep (betadine). Patient is in a side-lying position.
1510 First incision (only incision)
1515: camera inserted, initial chest cavity inspection, lung deflated. No significant adhesions or unexpected findings. Hilar dissection commences, with attention being given first to the pulmonary artery. By 1605, the left upper lobe branch of the pulmonary artery has been divided.
Dr. Gonzalez Rivas operating with Dr. Amore assisting. Dr. Casazza looks on.
1608: Bronchus stapled (resected). Patient noted to have an incomplete fissure of the upper lobe.
By 1612: The lobe is out. Dr. Gonzalez proceeds with radical lymph node dissection – including the nodes of the paratracheal area/ aortapulmonary window. The surgical field is essentially dry, with small amount of liquified fat from electrocautery dissection with just minor oozing from the aortopulmonary window. He places a small amount of surgicell in the subcarinal space, after harvesting several nodes to show the best angle of approach (posterior).
Dr. Gonzalez Rivas examines the lung specimen after removal
During surgery, he spends a few minutes demonstrating alternative techniques to hold and manipulate several instruments in one hand so that surgeons can minimize wasted movements.
After final inspection, Dr. Dario Amore assumes the role of primary surgeon – to place the chest tube (1653). Lung is re-inflated, and the ventilator/ respiratory loop is used to determine that there is no air leak. Camera out of the chest at 1655.
Vital signs: HR 76, NSR B/P 121/62 Sats 100% No hemodynamic instability or hypotension during the case. EBL for the case is around 90ml (+/- 10 ml due to lack of graduations on the suction canister).
Skin incision closed: 1710
By 1715: Patient is awake, extubated and able to verbal respond to commands/ questions.
**Since I was present in the operating room, I was privy to a great deal more information than audience members in the auditorium such as the pre-surgical patient review, monitor readings, etc.
Minimally invasive surgery course in Naples at Hospital Monaldi (April 23 – 24th, 2015)
Munich airport, Germany
I am on the last leg of a long journey to the beautiful southern Italian coastal city of Naples. Best known for its claim as the home of pizza and the nearby ruins of Pompeii, for the next few days, the department of thoracic surgery at Hospital Monaldi will be hosting surgeons (and one wee writer) from around the world for a two day course on minimally invasive and robotic surgery.
The event features live surgery demonstrations by Dr. Henrik Hansen and Dr. Diego Gonzalez Rivas, with a host of other speakers. For more details on the V corso VATS Monaldi Napoli dr Curcio dr Amore dr Casazza click the highlighted link for the full program.
Meanwhile, I will bring readers photos and highlights from the event.
As Dr. Gonzalez Rivas demonstrates, minimally invasive surgery isn’t just for “easy” cases. Case study with brief discussion and literature review
Uniportal VATS with chest wall resection at Shanghai Pulmonary Hospital
Shanghai, China
Authors: Gonzalez – Rivas, D. & Eckland, K.
Surgeons: Dr. Diego Gonzalez Rivas with Dr. Boxiong Xie assisting.
Case: 66-year-old patient with large left upper lobe mass extending into chest wall, biopsy proven carcinoma.
Pulmonary function tests – within acceptable margins
Imaging:
CT scan – showing a large left-sided lung upper lobe mass with chest wall invasion and rib involvement at the level just beneath the scapula.
Procedure: Uniportal (single incision) VATS with rib resection
Description: at a glance
Determining port placement
Due to tumor location, port placement had to be carefully considered and adjusted.
Vital signs at initiation of operation: HR 78, NSR B/P 95/56 Oxygen saturations: 100% (intubated with double lumen ETT)
First incision: 14:17
Making the initial incision
The tumor was adherent to the chest wall, requiring chest wall resection with rib resection.
performing uniportal VATS for tumor with chest wall invasion
The tumor was palpated thru the 2 cm incision allowing the surgeon the benefit of open surgery despite using a minimally invasive technique.
Palpating the tumor
Ribs were resected using a guillotine designed for minimally invasive use.
Rib resection
Lung resection complete at 17:42. The tumor was removed enblock using a bag system to prevent tumor spillage.
Tumor enblock after removal
Lymph node dissection completed at 17:56
There was a brief run of PVCs lasting about 30 seconds (B/P 83/54) with no desaturations. Patient was otherwise hemodynamically stable for the duration of the case.
Frozen section: clear pleural margins
EBL: 200ml
Discussion:
As noted by Pischik and others, many of the traditional contraindications for VATS procedures are no longer applicable, particularly for surgeons well versed in minimally invasive techniques like uniportal thoracoscopic surgery. In the case above, several of these contraindications were successfully addressed, including multiple adhesions, an incomplete interlobar fissure and a tumor with chest wall involvement.
That being said, this case was technically challenging from start to finish, due to the position of the chest wall tumor that required adjustment of port placement, a lengthy dissection of dense adhesions in addition to a sizeable chest wall mass. Hilar dissection was complicated by anatomical position, and the bronchus was difficult to access. This in addition to an incomplete fissure significantly lengthened the procedure.
VATS resection using a single port approach can be challenging even for experienced surgeons. However, it is a viable alternative for more complicated cases including those requiring a degree of chest wall resection.
This case was just one of numerous cases performed by Dr. Diego Gonzalez Rivas as part of the Uniportal VATS training course at Shanghai Pulmonary Hospital. Dr. Diego Gonzalez Rivas is the inventor of the uniportal technique and Director of Uniportal VATS training program at Shanghai Pulmonary Hospital. He has partnered with the Chinese facility to offer training courses for interested surgeons three times a year, in addition to his ‘wet-lab’ surgical training offerings in his home facility at La Coruna, Spain.
on location with Dr. Diego Gonzalez Rivas as he embarks on his latest project: teaching uniportal VATS to surgeons in China
Arriving at Wenzhou
Right now, I am on a Air China flight heading to Beijing after finishing up the first date on Dr. Diego Gonzalez Rivas, “7 Days, 7 Cities” Uniportal VATS instructional tour. I am here at the invitation of Dr. Gonzalez to chronicle the making of his second documentary film.
with Dr. Gonzalez Rivas and Spanish filmmaker, Danilo Lopez
Our first stop was Wenzhou, China where Dr. Gonzalez Rivas gave a lecture and performed a right middle lobectomy on a patient with a large lung lesion.
Dr. Gonzalez Rivas reviews patient films in consultation with local surgeons
It’s a different kind of experience for me, and it takes getting used to – knowing where NOT to stand, or walk so Danilo can get his shots. The whole live camera thing is a little bit off-putting. Everything is a production, nothing is left to chance. It can’t be – like the title of the film – it’s a fast trip, in and out. But it’s also an amazing experience. Danilo is amazingly talented (and very nice), and it’s hard to reconcile what looks like every day, run of the mill stuff with the footage he manages to capture. It’s strange and wonderful to see surgery thru his eyes. It’s also nice to have some camaraderie in the operating room as ‘media’.
The case went beautifully – another uniportal success story!
Dr. Gonzalez Rivas performing a surgical demonstration in Wenzhou, China
Goodbye Wenzhou – now off to Beijing!
**”I’m with the band” is my own lame joke because it says everything about my personality that I liken spending time in the operating room with a thoracic surgeon akin to traveling on the road with Mick Jagger back in his heyday.
the latest trailer about the documentary film on single port surgery and information about an upcoming training course.
For everyone that’s interested in learning more about the single port surgery technique, as taught by its creator, Dr. Diego Gonzalez Rivas – here’s another opportunity which may be closer to home for some readers.
Now, which way to Berlin?
The February conference takes place in Berlin, Germany on the 19th thru 21st. While Dr. Gonzalez Rivas, Dr. Delgado and Dr. Prado are headlining the event, other prominent thoracic surgeons such as Gaetano Rocco (Italy) and Alan Sihoe (Hong Kong) will also be lecturing at this event.
The conference includes live surgery demonstrations as well as a wet-lab for hands-on practice.
Deadline for registration is February 6th. Interested surgeons should contact:
R. Mette, M. Schmitt Charité – Universitätsmedizin Berlin Tel. +49 30 450 622 132 | Fax +49 30 450 522 929 E-mail: thoraxchiurgie@charite.de
In other news – the newest trailer for the documentary about Dr. Gonzalez Rivas and his work was recently released. I encourage all thoracic surgery personnel to see (and promote) this movie, which highlights the work of one of our own.
While Cirugia de Torax was unable to be in attendance and provide on location reporting and news, I would like to present some highlights from the recent event for our readers..
information about the upcoming VATS symposium in Cambridge, UK – with featured speakers Dr. Diego Gonzalez Rivas and Ian Hunt.
Another conference/ educational announcement for all residents, fellows and interested thoracic surgeons. This course is sponsored by the United Kingdom’s National Health Service and is being held in Cambridge, UK at Papworth Hospital this November. There is parallel content for nurses and other thoracic surgery personnel.
Internationally known Spanish surgeon Dr. Diego Gonzalez Rivas as well as native surgeon Mr. (Dr.) Ian Hunt of St. George’s Hospital in London, will be part of the faculty teaching this course.
Dr. Gonzalez Rivas will be discussing single port surgery in addition to performing a live case on the second day of the symposium.
Mr. Hunt will be discussing how to perform a total lymphadenectomy, as well as lymphadenectomies on more complicated cases.
Additional speakers will be discussing topics including issues in thoracic anesthesia, management of bleeding (in VATS and other minimally invasive surgery), and managing other operative complications.
a new film showing the life-changing efforts of one thoracic surgeon.. It’s about time!
Dr. Diego Gonzalez Rivas
I am excited beyond words to hear that my long-time hero and champion of modern-day thoracic surgery, Dr. Diego Gonzalez Rivas, is featured in a new documentary film, “This is Life”. The film follows the life of a patient undergoing a single incision thoracoscopic lobectomy. The film is being released this December.
I eagerly await the film – and am happy to see thoracic surgery (and Dr. Diego Gonzalez Rivas) get their due. For too long, our humble specialty has been overlooked for the more ‘glamorous’ cardiac surgery. This oversight has led to a dire shortage of thoracic surgeons in many parts of the world.
Hopefully, this is only part of an ongoing effort to have thoracic surgery recognized as an independent and complex surgical specialty requiring extensive knowledge, advanced skills and training. It is not an ‘add-on’ for cardiac surgeons with insufficient cardiac consultations.
Dr. Gonzalez Rivas and single-port surgery in Shanghai, China
For those of you hoping to see – and learn from the best, Dr. Gonzalez Rivas will be spending much of the month of October in Shanghai, China at the “National Uniportal VATS Training Course & Continuing Medical Education Forum on General Thoracic Surgery” which runs from October 8th to November 8th, 2014 at Tongi University.
Alas! To my eternal regret, Cirugia de Torax will not be in attendance. However, I will have sources on the ground – and hope to post more information during the conference,
Talking about the roles of traditional VATS, single port surgery and robots in modern thoracic surgery.
The Ethicon (Johnson & Johnson) sponsored session was by far, the best of the conference – and an excellent overview of modern technologies in thoracic surgery.
starting with Dr. Ricardo Buitrago (purple tie), Dr. Diego Gonzalez Rivas (blue tie) and Dr. Mario Ghefter (pink tie) are changing the future of thoracic surgery
Dr. Diego Gonzalez Rivas
“Is uni-port surgery feasible for advanced cancers?” Short answer: Yes.
The first speaker, was Dr. Diego Gonzalez Rivas of Coruna, Spain. He is a world-renown thoracic surgeon and innovator of uni-port thoracoscopic surgery. He discussed the evolution of single port surgery as well as the most recent developments with this technique, including more advanced and technically challenging cases such as chest wall resections (2013), sleeve resections/ reconstructions (2013), pulmonary artery reconstructions (2013) and surgery on non-intubated, awake patients (2014).
Experience and Management of bleeding
The biggest challenges to surgeons learning this technique is management of bleeding. But as he explained in previous lectures, this can be overcome with a direct approach. (these lectures and YouTube videos, Dr. Gonzalez explains the best ways to manage intra-operative bleeding.) In the vast majority of cases – this did not require deviation or conversion from the uni-port technique.)
As surgeons gain proficiency with this technique which mirrors open surgery, the only contra-indications for surgical resection of cancerous tissue (by single port) are tumors of great size, and surgeon discomfort with the technique.
Dr. Mario Ghefter
My favorite lecture of the series was given by Dr. Mario Ghefter of Sao Paolo, Brazil. While his lecture was ostensibly about video-assisted thoracoscopy (VATS), it was more of a retrospective vision and discussion of the modern history of thoracic surgery as seen through the eyes of a 22 year veteran surgeon.
He talked about the beginnings of VATS surgery and the contributions from such legends as Cefolio and D’Amico, including the 2005 paper – and modern-day thoracic bible, “Troubleshooting video-assisted thoracoscopic lobectomy (Demmy, James, Swanson, McKenna and D’Amico).
Dr. Ghefter also talked about how improved imaging and diagnostic procedures such as PET-CT and EBUS have been able to provide additional diagnostic information pre-operatively that helps surgeons to plan their procedures and treatment strategies more effectively.
Dr. Mario Ghefter
As a counterpoint to both Dr. Gonzalez and Dr. Buitrago, Dr. Ghefter acquitted himself admirably. He reminded audience members that even the newer technologies have some drawbacks – both as procedures and for the surgeons themselves.
He also successfully argued (in my opinion) that while the popularity of procedures such as multiple port VATS and even open thoracotomies have dropped drastically as thoracic surgeons embrace newer technologies, there will always be a place and time for these more traditional procedures.
Dr. Mario Ghefter is the Director of Thoracic Surgery at Hospital do Servidor Público Estadual – Sāo Paulo and on staff at the Hospital Alemão Oswaldo Cruz.
Dr. Ricardo Buitrago
Native Colombian (and my former professor), Dr. Ricardo Buitrago is acknowledged as one of the foremost experts in robotic thoracic surgery in Latin America.
During his presentation, he discussed the principles and basics of use of robotic techniques in thoracic surgery. He reviewed the existing literature surrounding the use of robotic surgery, and comparisons of outcomes between thoracic surgery and traditional lobectomy.
He reviewed several recent robotic surgery cases and the use of robotics as a training tool for residents and fellows.
While he mentioned some of previously discussed limitations of robotic surgery (namely cost of equipment) he cited recent studies demonstrating significant cost savings due to decreased length of stay and a reduced incidence of surgical complications.
He also discussed recent studies (by pioneering surgeons such as Dr. Dylewski) demonstrated short operating times of around 90 minutes.
the Babe Ruth of thoracic surgery continues his winning streak; and Dr. Benny Weksler heads south to the University of Tennessee. Kudos to both of these fine surgeons!
It’s another home run for Dr. Gonzalez Rivas as he and his team perform a single port (uni-port) thoracoscopic lobectomy with under local anesthesia, as reported by a recent story, “Operan un tumor e pulmón con una sola incisión y anestesia local” by Raul Romar in La Voz de Galicia.
Dr. Gonzalez Rivas demonstrates uniportal VATS
The answer is International collaboration and sharing of ideas
Dr. Gonzalez Rivas is used to sharing his ideas. After all, he spends a considerable amount of time traveling the world doing just that; sharing information about and teaching surgeons how to perform the single port thoracoscopic technique. But that doesn’t mean that he does find time to learn from his peers during his travels.
The article above highlights the importance of this international collaboration as it details how Dr. Gonzalez Rivas began to consider applying a local anesthesia approach to the single port surgical technique after talking (and visiting) surgeons in Taiwan and China.
Once he found the perfect candidate, he was ready to implement local anesthesia into his single port approach.. The rest, as they say – is now headed for the Annals of Thoracic Surgery.
Click here for English translation (note translation is not exact).
Dr. Benny Weksler, our own American (via Brazil) superstar surgeon recently made the move to the University of Tennessee. Dr. Weksler made the move in November of 2013 and is now settling in to his new position as Chief of Thoracic Surgery for the University of Tennessee (UT) Health Science Center and UT – Methodist.
Dr. Weksler, one of the United States most prominent thoracic surgeons, particularly in the area of esophageal surgery reports that he has big plans for the UT health system and the thoracic surgery department.
Big Plans for UT and the city of Memphis
These plans include a lung cancer screening program targeting vulnerable populations in Memphis including the uninsured/ underinsured, African-Americans (who are disproportionately affected) and smokers.
Related: Dr. Weksler talks about smoking cessation
Minimally invasive techniques for esophageal surgery
He has also started a new minimally invasive esophageal surgery program for esophageal cancer and reports “that there is almost an epidemics of squamous cell carcinoma of the esophagus” which is something tha was more rare in his previous practice in Pittsburgh, Pennsylvania.
Dr. Weksler and his colleagues are putting together a multi-disciplinary treatment plan to try to get these patients to a complete evaluation with a surgeon, an oncologist, and a radiation oncologist to provide patients with comprehensive, multi-faceted and coördinated care.
“The Surgeon Speaks” – Dr. Weksler talks about robotic surgery in this 2009 Jefferson University publication.
As a former Memphis resident, I want to say, “Welcome to the mid-south.. Hope you find time in your busy schedule to enjoy Beale Street, visit the Pink Palace and tour Graceland.. On behalf of all current Memphians, we are glad you are here.”
*This article was written by the author of this post.
the latest from Dr. Diego Gonzalez Rivas and the masters of thoracic surgery.
Dr. Gonzalez Rivas and the Thoracic Surgery Unit in Coruna, Spain are hosting the “International Symposium on Uniportal VATS” this week (February 26th to 28th, 2014).
Dr. Gonzalez Rivas demonstrates uniportal VATS
While the in-person, on-site event is limited to just 100 attendees, the event will be offering real-time live streaming surgery for viewers worldwide.
With registrations from around the world, Dr. Gonzalez Rivas estimates that thousands of pairs of eyes will be watching; from Australia to Saudi Arabia, Hong Kong to Colombia, Brazil to Russia, and the United States.
If you’ve ever wanted to learn more about single port VATS, this is the time to find out.
For more information:
Livethoracic.com – link to the event and on-line registration. Registration is 500 Euros.
Article at Examiner.com with more details on this event.
Dr. Diego Gonzalez Rivas receives recognition from the global network of cardiothoracic surgeons, CTSnet.
CTSnet.org, the largest global network of cardiothoracic surgery professionals has recently recognized Dr. Diego Gonzalez Rivas for his pioneering efforts in thoracic surgery.
a TEDtalk favorite
This comes on the heels of a recent TEDtalk on Dr. Gonzalez and the process of innovation in surgery. During this 18 minute talk, Dr. Gonzalez talks about his own experiences in surgery.
Dr. Diego Gonzalez Rivas, a “fan” favorite here at Cirugia de Torax, is at the forefront of the field due to his contributions to minimally invasive surgery in the area of single-port thoracoscopy.
The dynamic young Spaniard has been making headlines over the last decade as he introduced and then refined the single port surgical technique. He and his colleagues, Dr. Maria Mercedes
de la Torre Bravos and Dr. Ricardo Fernandez Prado at the Minimally Invasive Thoracic Surgery Unit (UCTMI) in Coruna, Spain have successfully used this technique on thousands of patients, for a wide variety of procedures including sleeve lobectomies, pneumonectomies, bilobectomies and other complex procedures.
Dr. Gonzalez-Rivas demonstrates single port thoracoscopy at the National Cancer Institute in Bogotá, Colombia
Despite this widespread fame, Dr. Gonzalez Rivas remains unaffected and approachable. He spends much of his time in operating rooms around the world, teaching his technique to his peers. Next week, he heads to Guangzhou, China.
Some of the biggest names in thoracic surgery were in attendance, to present their research and surgical techniques to a crowd of over 600 Chinese thoracic surgeons. The lectures (and live surgery) were also broadcast across China.
World-renown thoracic surgeons at the 16th National Forum in Shanghai, China
Invited International Speakers included:
Dr. G. Alexander Patterson, thoracic surgeon/ lung transplant from the Washington School of Medicine in St. Louis, Mo. (USA). Dr. Patterson gave a lecture on clinical experiences and advances in Lung Transplantation. He also lectured on pancoast tumors.
Dr. Claude Deschamps, French Canadian thoracic surgeon and Chair of Surgery at the Mayo Clinic, Rochester, MN (USA). Dr. Deschamps talked about the use of anti-reflux surgery.
Dr. Gaetano Rocco, of the National Cancer Institute in Naples, Italy. Dr. Rocco talked about advances in chest wall reconstruction. He gave another lecture on uniport surgery.
Dr. Alan Sihoe from the University of Hong Kong discussed management of air leaks.
Surgeons from Taiwan and mainland China presented on a variety of topics including tracheal surgery, management of empyema, sympathectomy for hyperhidrosis and surgical treatment of tuberculosis. (The full list of speakers and topics presented is available here*.)
Conference Spotlight: Single port surgery
But the focal point of the forum was single port (uniportal) surgery. Saturday (the 19th) was devoted to lectures and demonstrations of the single port thoracoscopic technique, including live surgical demonstrations performed by Dr. Diego Gonzalez Rivas. His live surgery presentation was viewed by 500 surgeons at the conference as well as hundreds of other surgeons via a live feed.
Dr. Gonzalez Rivas demonstrates the single port (uniport) technique in Shanghai, China
Thank you to Dr. Gonzalez Rivas for his submission. We welcome reports, photographs and discussions on recent and upcoming thoracic surgery conferences. If you have a meeting, paper or presentation to share, please contact us at k.eckland@gmail.com
*Information is translated from Mandarin using google software with some obvious translational errors, particularly names of several of the Chinese surgeons.
the 2013 S.W.A.T conference, presented by Johnson & Johnson. Featured presenters Dr. Diego Gonzalez Rivas and Dr. Paula Ugalde discuss single port thoracoscopy and topics in minimally invasive surgery
Very pleased that despite the initial difficulties, we are able to provide information regarding the recent conference.
Talking about Single-port surgery in Bogotá, Colombia – 2013 S.W.A.T. Summit
Dr. Diego Gonzalez Rivas and Dr. Paula Ugalde were the headliners at the recent Johnson and Johnson thoracic surgery summit on minimally invasive surgery. Both surgeons gave multiple presentations on several topics. They were joined at the lectern by several local Colombian surgeons including Dr. Stella Martinez Jaramillo (Bogotá), Dr. Luis Fernando Rueda (Barranquilla), Dr. Jose Maineri (Venezuela) Dr. Mario Lopez (Bogotá) and Dr. Pardo (Cartagena).
Thoracic surgeons at the 2013 S.W.A.T Summit in Bogota, Colombia. Drs. Gonzalez-Rivas and Dr. Paula Ugalde are center, front-row
Target audience missing from conference
The audience was made up of thirty Latin American surgeons from Colombia, Costa Rica and Venezuela. This surgeons were hand-picked for this invitation-only event. Unfortunately, while Johnson and Johnson organized and presented a lovely event; their apparent lack of knowledge about the local (Colombian) thoracic surgery community resulted in the exclusion of several key surgeons including Dr. Mauricio Velasquez, one of Colombia’s earliest adopters of single-port thoracoscopy. Also excluded were the junior members of the community, including Dr. Castano, Dr. Carlos Carvajal, and current thoracic surgery fellows. It was an otherwise outstandingand informative event.
The Gonzalez – Rivas dissector, photo courtesy of Scanlon International
As discussed in multiple publications, previous posts as well as during the conference itself, it is these younger members who are more likely to adopt newer surgical techniques versus older, more experienced surgeons. More seasoned surgeons may be hesitant to change their practices since they are more comfortable and accustomed to open surgical procedures.
Despite their absence, it was an engaging and interesting conference which engendered lively discussion among the surgeons present.
Of course, the highlight of the conference actually occurred the day before, when Dr. Gonzalez- Rivas demonstrated his technique during two separate cases at the National Cancer Institute in Bogotá, Colombia. (Case report).
Dr. Gonzalez-Rivas and Dr. Ricardo Buitrago performing single port thoracoscopy at the National Cancer Institute
Featured presenters:
Dr. Diego Gonzalez – Rivas is a world-renown thoracic surgeon jointly credited (along with Dr. Gaetano Rocco) with the development of single-port thoracoscopic (uni-port) surgery. He and his colleagues at the Minimally Invasive Surgery Unit in La Coruna, Spain give classes and lectures on this technique internationally. Recent publications include three papers in July alone detailing the application of this surgical approach, as well as several YouTube videos demonstrating use of this technique for a wide variety of cases.
Dr. Gonzalez Rivas
Dr. Paula Ugalde, a Chilean-borne thoracic surgeon (from Brazil) who gave several presentations on minimally-invasive surgery topics. She is currently affiliated with a facility in Quebec, Canada.
Dr. Paula Ugalde
Refuting the folklore
Part of the conference focused on refuting the ‘folklore’ of minimally-invasive procedures. Some of these falsehoods have plagued minimally-invasive surgery since the beginning of VATS (in 1991), such as the belief that VATS should not be applied in oncology cases. The presenters also discussed how uniportal VATS actually provides improved visibility and spatial perception over traditional VATS (Bertolaccini et al. 2013).
However, Gonzalez-Rivas, Ugalde and the other surgeons in attendance presented a wealth of data, and publications to demonstrate:
– VATS is safe and feasible for surgical resection in patients with cancer. (Like all surgeries, oncological principles like obtaining clear margins, and performing a thorough lymph node dissection need to be maintained).
– Thorough and complete lymph node dissection is possible using minimally invasive techniques like single-port surgery. Multiple studies have demonstrated that on average, surgeons using this technique obtain more nodes than surgeons using more traditional methods.
– Large surgeries like pneumonectomies and sleeve resections are reasonable and feasible to perform with single-port thoracoscopy. Using these techniques may reduce morbidity, pain and length of stay in these patients.
– Rates of conversion to open surgery are very low (rare occurrence). In single-port surgery, “conversion” usually means adding another port – not making a larger incision.
– Learning curve fallacies: the learning curve varies with each individual surgeon – but in general, surgeons proficient in traditional VATS and younger surgeons (the “X box generation”) will readily adapt to single-port surgery.
– Bleeding, even significant bleeding can be managed using single-port thoracoscopy. Dr. Gonzalez Rivas gave a separate presentation using several operative videos to demonstrate methods of controlling bleeding during single-port surgery – since this is a common concern among surgeons hesitant to apply these advanced surgical techniques.
Additional References / Readings about Single-Port Thoracoscopy
Scanlon single-port thoracoscopy kits – informational brochure about specially designed instruments endorsed by Dr. Gonzalez Rivas.
Dr. Diego Gonzalez Rivas – YouTube channel : Dr. Gonzalez Rivas maintains an active YouTube channel with multiple videos demonstrating his surgical technique during a variety of cases. Below is a full-length video demonstrating the uniportal technique.
Additional posts at Cirugia de Torax about Dr. Diego Gonzalez- Rivas
Upcoming conference in Florida – information about registering for September conference for hands-on course in single-port thoracoscopic surgery with Dr. Gonzalez-Rivas
Youtube video for web conference on Single-port thoracoscopic surgery
Bertolaccini, L., Rocco, G., Viti, A. & Terzi, A. (2013). Surgical technique: Geometrical characteristics of uniportal VATS. J. Thorac Dis. 2013, Apr 07. Article from thoracic surgeons at the National Cancer Institute in Naples, Italy explains how the geometric advantages of uniportal VATS improves visibility and spatial perception over traditional VATS, and mimics open surgery.
Calvin, S. H. Ng (2013). Uniportal VATS in Asia.J Thorac Dis 2013 Jun 20. Article discussing the spread of uniportal techniques in Taiwan, China and other parts of Asia.
Rocco, G. (2013). VATS and uniportal VATS: a glimpse into the future.J. Thorac Dis. 2013 July 04. After coming across several articles by Dr. Gaetano Rocco, and actively pursuing several other publications by this Italian thoracic surgeon, I have become increasingly convinced that Gaetano Rocco, along with Dr. Gonzalez Rivas is one of the world’s leading innovators in thoracic surgery. Hopefully, cirugia de torax will be able to catch up to Dr. Rocco at some point for an in-depth discussion.
While I advance criticism of this event – it was a fantastic conference. My only reservations were to the exclusivity of the event. While this was certainly related to the costs of providing facilities and services for this event – hopefully, the next J & J thoracic event will be open to more interested individuals including young surgeons and nurses.
writing about Dr. Diego Gonzalez Rivas and the other living legends in thoracic surgery and connecting people to the world of thoracic surgery
Readers at Cirugia de Torax have certainly noticed that there are numerous articles regarding the work of Dr. Diego Gonzalez Rivas. This week in particular, after a recent thoracic surgery conference and an afternoon in the operating room – there is a lot to say about the Spanish surgeon.
It’s also hard to escape that fact that I regard him in considerable awe and esteem for his numerous contributions to thoracic surgery and prolific publications. I imagine that this is similar to how many people felt about Drs. Cooley, Pearson or Debakey during their prime.
Making thoracic surgery accessible
But the difference is Dr. Diego Gonzalez Rivas himself. Despite the international fame and critical surgical acclaim, he remains friendly and approachable. He has also been extremely supportive of my work, at a time when not many people in thoracic surgery see the necessity or utility of a nurse-run website.
After all, the internet is filled with other options for readers; CTSnet.org, multiple societies like the Society of Thoracic Surgeons (STS), and massive compilations like journal-based sites (Annals of Thoracic Surgery, Journal of Thoracic Disease, Interactive Journal of Cardiothoracic Surgery).
But the difference between Cirugia de Torax and those sites is like the difference between Dr. Gonzalez Rivas and many of the original masters of surgery: Approach-ability and accessibility.
This site is specifically designed for a wider range of appeal, for both professionals in thoracic surgery, and for our consumers – the patients and their families. Research, innovation, news and development matters to all of us, not just the professionals in the hallowed halls of academia. But sometimes it doesn’t feel that way.
Serving practicing surgeons
For practice-based clinicians, and international surgeons publication in an academia-based journal requires a significant effort. These surgeons usually don’t have research assistants, residents and government grants to support their efforts, collect their data and clean up their grammar. Often English is a second or third language. But that doesn’t mean that they don’t make valuable contributions to their patients and the practice of thoracic surgery. This is their platform, to bring their efforts to their peers and the world.
Heady aspirations
That may sound like a lofty goal, but we have readers from over a 110 countries, with hundreds of subscribers along with over 6,000 people with Cirugia de Torax directly on their smart phone. Each month, we attract more hits and more readers.
Every day, at least 200 people read “Blebs, Bullae and Spontanous Pneumothorax”. Why? Because it’s a concise article that explains what blebs are, how a pneumothorax occurs and how it’s treated. Another hundred people usually go on to read the accompanying case report about blebectomy, for similar reasons. There are links for more information, CT scans and intra-operative photos included, so that people can find exactly what they need with a minimum of effort.
Avoiding ‘Google overload’
With the massive volume of information available on the internet, high-quality, easily understood, applicable information has actually become even more difficult for patients to find than ever before. Patients spend hours upon hours browsing through academic jargon, commercial websites and biased materials while attempting to sift through the reams of information for pertinent and easily understandable information. There is also a lot of great material out there – so we provide links to reputable sites, recommend well-written articles and discuss related research.
Connecting patients to surgeons
We also provide patients with more information about the people they are entrusting their bodies, their hopes and their lives to. It’s important that they know about the Dr. Benny Wekslers, the Dr. Hanao Chens, and the Dr. Diego Gonzalez Rivas out there.
Update: June 2019
After multiple reader requests from this site, we have launched a service to assist readers in pursuiting minimally invasive thoracic surgery, uniportal surgery, HITHOC and other state-of-the-art thoracic surgery procedures with the modern masters of thoracic surgery. We won’t talk a lot about this on the site, but we do want readers to know that we are here to help you. If you are wondering what surgery costs like with one of the world’s experts – it’s often surprisingly affordable.
If you are interested in knowing more, please head to our sister site, www.americanphysiciansnetwork.org or send an email to kristin@americanphysiciansnetwork.org.
Keeping it ‘real’
Looking over the shoulder of Dr. Gonzalez Rivas in the operating room
As much as I may admire the work and the accomplishments of Dr. Gonzalez-Rivas – it’s important not to place him on a pedestal. He and his colleagues are real, practicing surgeons who operating on regular people, not just heads of state and celebrities. So when we interview these surgeons and head to the OR, it’s time to forget about the accolades, the published papers and the fancy titles. It’s time to focus on the operations, the techniques, the patients and the outcomes because ‘master of thoracic surgery’ or rural surgeon – the operation and patient are all that really matters.
For thoracic surgeons interested in becoming more familiar with uniport surgery, this is your chance to learn from the pioneers of the technique.
Several new dates for Uni-port thoracoscopy with Dr. Diego Gonzalez Rivas. These events span across the Americas and Europe, so if you are interested in uni-port thoracoscopic surgery, then there is something nearby.
The first date is coming up soon – in August 2013, in Bogotá, Colombia.
Dr. Diego Gonzalez Rivas in Bogotá, Colombia
I am excited about this one, and hope to be able to cover the event for readers of CdeT. While I am currently in Medellin, I became familiar with, (and have a great deal of respect for) many of Bogotá’s finest thoracic surgeons in the past so it’s a great opportunity not just to hear more about Dr. Diego Gonzalez Rivas and uni-port thoracoscopy but to check in local surgeons and hear about some of their more interesting cases.
Dr. Gonzalez will be joined by Dr. Paula Ugalde, a well-known thoracic surgeon from Brazil (now practicing in Quebec, Canada).
As soon as I get some more details on the Bogotá event – I’ll post them here..
Split, Crotia – September 12th – 15th – 23rd Congress of the World Society of Cardio-Thoracic Surgeons.
This conference is being jointly sponsered by the Society of Cardio-Thoracic Surgeons of South Africa (SCTSSA). Dr. Diego Gonzalez will be talking about “Uni-port VATS major pulmonary resections in advanced lung cancer” in an afternoon session on September 13, 2013. (Obviously they don’t know much about him – since it’s only a 20 minute session – but as a CTS conference, only about 10% is thoracic topics (he is one of just a handful of thoracic speakers.)
Then in mid -September 2013, he will part of a roster of the greats of thoracic surgery (Dr. Robert Cefolio, Dr. James Luketich and Dr. Thomas D’Amico) at the Duke Center for Surgical Innovation for a course entitled, “Masters of Minimally Invasive Thoracic Surgery”.
The second event, is a meeting/ conference/ training course in Dr. Gonzalez’s home hospital in Coruna, Spain. The event, “Live Thoracic” will feature ‘live-surgery’ demonstrations and will be streamed for real-time viewing from around the world.
In a side note – I want to thank the nearly 6,000 students, interns, nurses, residents and thoracic surgeons who have downloaded one of my thoracic surgery apps for Android devices.
the latest video from Dr. Diego Gonzalez Rivas demonstrating a sleeve lobectomy via single port surgery
On the heels of the recent conference in Hong Kong, one of our favorite surgeons (and presenter at the 1st Asian single port surgery conference), Dr. Diego Gonzalez Rivas has sent another link to one of his more recent cases – Single port lobectomy – Sleeve resection after chemotherapy.
Gonzalez Rivas, D. (2013). Evolving thoracic surgery: from open surgery to single port thoracoscopic surgery and future robotic. Chinese Journal of Cancer Research, 25 (1) 4-6. Editorial pdf download.
Interested in learning more about single port thoracoscopy, or talking to the inventors of this technique? This March – head to the 1st Asian single port surgery conference in Hong Kong.
It doesn’t look like Cirugia de Torax will be in attendance for this conference, but it’s another opportunity for practicing thoracic surgeons and thoracic surgery fellows to learn more about single port thoracoscopic surgery.
This March (7th – 8th), the Chinese University of Hong Kong, along with the Minimally Invasive Thoracic Surgery Unit (Coruna, Spain), and Duke University are presenting the 1st Asian Single Port Symposium and Live Surgery conference in Hong Kong.
This is your chance to meet the experts – and the inventors of this technique (such as Dr. Diego Gonzalez – Rivas, one of the new masters frequently featured here at Cirugia de Torax.)
an Interview with Dr. Diego Gonzalez Rivas – and coverage of ‘Videotoracoscopia y cirugia robotica en torax: Avances y perspectivas’ in Santiago, Chile
Santiago, Chile
I was a little intimidated to actually interview Dr. Diego Gonzalez Rivas after reading his articles and pestering him with emails for the last few years. But he was just as nice and patient with my questions as he’s always been.
Dr. Santolaya, Dr. Sales dos Santos, Dr.Berrios and Dr. Diego Gonzalez Rivas
Since publishing the last few articles on his single port technique, Dr. Gonzalez has been in high demand from thoracic surgeons wanting to learn more, and to train in single port techniques. In addition to traveling the world to teach – he continues to offer training at the Minimally Invasive Thoracic Surgery Unit at the Complexo Hospitalario Universitario de A Coruna, in Coruna, Spain.
Dr. Gonzalez reports that single port thoracoscopy doesn’t just provide patients with the least invasive surgery possible, but that single port thoracoscopy is superior to traditional VATS in the vast majority of cases. Single port thoracoscopy is defined by the creation of one 2cm to 4cm incision – with no rib spreading and utilization of video-assisted thoracoscopy.
“Forward Motion”
He states that using a single port approach gives much better visibility than traditional VATS. This visibility is equal to that of open surgery – versus the 3 or 4 port approach, which is constrained by the 30 degree movement / rotation of the thoracoscope. This visibility concept; called ‘Forward Motion,’ along with the ease of using instrumentation through the same port makes single port surgery amendable to most thoracic surgery procedures.
Learning curve? What learning curve?
He reports that members of the “Playstation Generation” as he terms the newest young surgeons, adapt more readily to the use of both traditional and single port thoracoscopy. In fact, he reports that the residents (in his program) are able to learn and use this approach with minimal assistance.
With the exception of lung transplantation (requiring the traditional clamshell incision), Dr. Gonzalez reports that he is able to successfully perform a wide range of surgeries from wedge resections and lobectomies to more complicated procedures such as pneumonectomies and sleeve resections.
In today’s lecture he debunks some of the myths regarding the ‘classic contraindications’ to video-assisted thoracoscopy (VATS) such as broncheoplasty, the presence of dense adhesions or the need for complete lymph node dissection. While he reports that dense adhesions may make the procedure more painstaking and difficult – it is still possible.
LymphNode Dissection
In cases of lymph node dissection – he reports that lymphadenectomy is actually superior by single port and other VATS methods, with the average surgeon actually harvesting more nodes, more easily.
While he initially believed that right upper lobe resections would be impossible with this method – his recent experiences (included in an upcoming paper on 102 cases) show that any anatomic complexities are readily overcome by an experienced VATS surgeon. Not only that, but he has been able to successfully remove very large (8cm or greater) lung tumors using this method – by slightly enlarging the port at the time of specimen removal. He has also successfully removed Pancoast tumors and performed chest wall resections with this procedure, as well as single port thoracoscopy after previous VATS or previous thoracotomy including completion pnuemonectomies and completion sleeve lobectomies.
One of the biggest obstacles for surgeons implementing the single port method is the dreaded complication of catastrophic bleeding. This often causes inexperienced single port surgeons to hasten to convert to open surgery without attempting to control the bleeding. Dr. Gonzalez presented several cases today to demonstrate the difference between controlled bleeding that can be managed with the speedy application of surgical staples, clips or sutures versus heavy uncontrolled bleeding, which requires quick recognition and prompt conversion to open thoracotomy.
He reports that in the over 500 cases he has performed by VATS (3 port, dual port and single port), conversion to open thoracotomy remains a very rare occurence. (He presented data on his outcomes today.)
In his own practice, he reports that prior to 2007 the majority of cases were by traditional thoracotomy. He began using 3 port VATS more heavily in 2007 – 2009. After training with Dr. D’Amico at Duke University in Durham, NC – he moved to dual port thoracoscopy in 2009. Since 2010, his practice is almost exclusively single port thoracoscopy.
The future of single port thoracoscopy
Dr. Gonzalez believes the future of single port thoracoscopy will be a hybridization of current robotic thoracic surgery (which now uses three and four port techniques) to using less invasive, smaller robotic arms that will allow surgeons to enjoy the micro-precision of robotic technology through a single port.
Not just a ‘single port surgeon’
While he is famous internationally for his innovations in the field of minimally invasive surgery, he is also a transplant surgeon. In fact, along with his partners, he performed an average of 35 – 40 lung transplants a year.* This makes the transplant program in Coruna the second largest in Spain, despite the relatively small size of Coruna compared to other cities such as Barcelona or Madrid.
For patients who are interested in Dr. Gonzalez-Rivas and his program, please contact him at Info@videocirugiatoracica.com
I published an article based on this interview over at Examiner.com
5 / Video-assisted thoracic surgery lobectomy: 3-year initial experience with 200 cases. Gonzalez D, De la Torre M, Paradela M, Fernandez R, Delgado M, Garcia J,Fieira E, Mendez L. Eur J Cardiothorac Surg. 2011 40(1):e21-8.
6 / Single-port Video-Assisted Thoracoscopic Anatomical Resection: Initial Experience. Diego Gonzalez , Ricardo Fernandez, Mercedes De La Torre, Maria Delgado, Marina Paradela, Lucia Mendez. Innovations.Vol 6.Number 3. May/jun 2011. Page 165.
Books/ Book Chapters
1 / Thoracoscopic lobectomy through a single incision. Diego Gonzalez-Rivas, Ricardo Fernandez, Mercedes de la Torre, and Antonio E. Martin-Ucar. Multimedia Manual of Cardio-Thoracic Surgery. MMCTS (2012) Vol. 2012 doi:10.1093/mmcts/mms007. Includes multiple videos demonstrating single port techniques.
2 / Tumores del diafragma. M. de la Torre Bravos, D. González Rivas, R. Fernández Prado, JM Borro Maté. Tratado de Cirugía Torácica. Editores L. Fernandez Fau, J. Freixinet Gilart. SEPAR Editores médicos SA. Madrid 2010. Vol 2, Sec VIII, Capitulo 87: 1269-78.
3 / Trasplante Pulmonar. C. Damas, M. De la Torre, W. Hespanhol, J.M. Borro. Atlas de Pneumología. Editores A. Segorbe Luís y R. Sotto-Mayor 2010. Vol 2, Capítulo 54 651-8.
4 / Doble utilidad hemostática y sellante de fuga aérea de tachosil en un caso de cirugía compleja por bronquiectasias. M. De la Torre, J.M. Borro, D. González, R. Fernández, M. Delgado, M. Paradela. Anuario 2009. Casos clínicos en cirugía. Accesit en la 3ª edición de los Premios Nycomed 2008.
5 / Cirugía Torácica videoasistida avanzada. D. González Rivas. Videomed 2008. Certamen internacional de cine médico y científico.
6 / Traumatismo Torácico. M. de la Torre, M. Córdoba. En « Manual de Urgencias en Neumología». Editado por Luis M Domínguez Juncal, 1999 165-78.
7 / Neumotórax. M. Córdoba, M. de la Torre. En « Manual de Urgencias en Neumología». Editado por Luis M Domínguez Juncal, 1999 139-56.
8 / Cirugía del enfisema. P. Gámez, J.J. Rivas, M . de la Torre. En « Neumología Práctica al Día». Boehringer Ingelheim 1998 77-102.
9 / Neumotórax. J.J. Rivas, J. Torres, M. de la Torre, E. Toubes. En « Manual de Neumología y Cirugía Torácica». Editores Médicos S.A. 1998 1721-37.
Checking in with Dr. Diego Gonzalez – Rivas and his team in Coruna, Spain – the innovators in single incision thoracic surgery, as Dr. Gonzalez publishes a new report on single incision pneumonectomy.
After speaking with Dr. Raimundo Santolaya last week – I contacted Dr. Diego Gonzalez over at UTCMI in Coruna, Spain to see what he’s been doing since our last contact, and discuss a possible interview in the future.
Last fall, he published another case report on single incision VATS – lobectomy, and since then he has continued to operate and publish reports on his successes. Now he has an upcoming case report on a right-sided single-port pneumonectomy, which was largely held as one of the last frontiers in VATS procedures. (Pneumonectomy by standard VATS, despite being reported in the literature several years ago, remains a relatively uncommon procedure.)
While a common criticism of his work is related to the fact that removing a portion of the lung as large as a lobe, or an entire lung requires a small additional incision at the conclusion of the case – but these criticisms are weak at best – and fail to see the true clinical importance of his continued innovation and investigation in advancing video-assisted thoracoscopic surgery for the benefits of our patients. Ten years from now – single incision VATS will be a common procedure, and Drs. Gonzalez, Fernandez and De la Torre will be the ones responsible.
References: Single port pneumonectomy
Gonzalez-Rivas D, de la Torre M, Fernandez R, Garcia J. (2012). Single-incision video-assisted thoracoscopic right pneumonectomy. Surg Endosc. 2012 Jan 11. [Epub ahead of print – abstract re-posted below]
Abstract
BACKGROUND:The most common approach for Video-assisted thoracoscopic (VATS) lobectomy is undertaken with three or four incisions, including a utility incision of about 3-5 cm. However, major pulmonary resections are amenable by using only a single utility incision. This video shows the technical procedure of a right pneumonectomy by single-incision approach with no rib spreading.
METHODS: A 52-year-old woman was proposed for single-incision VATS resection of a 5-cm right lower lobe adenocarcinoma. A 4-cm incision was made in the fifth intercostal space. We placed a 30-degree, high-definition, 10-mm thoracoscope in the posterior anterior part of the incision. Digital palpation confirmed that the tumor involved the fissure and the posterior portion of the upper lobe, which indicated the need for right pneumonectomy. We inserted the instruments through the anterior part of the utility incision to start the detachment of the right upper lobe by using a harmonic scalpel. The first step was dissecting the inferior pulmonary vein. The hilar structures were exposed by using harmonic scalpel and a long dissector (Fig. 1A). The upper and middle-lobe pulmonary veins were dissected and transected, allowing visualization of truncus anterior, which was then stapled. The inferior pulmonary vein and the intermediate truncus artery were divided, allowing optimal exposure to the main bronchus, which was stapled. The lung was removed in a protective bag by adding 1 cm to the incision, and a systematic lymph node dissection was performed. A single chest tube was placed in the posterior part of the utility incision.
RESULTS: Total surgery time was 210 min. The chest tube was removed on postoperative day 2, and the patient was discharged home on day 4 with no complications.
CONCLUSIONS: Single-port VATS pneumonectomy for selected cases is a feasible procedure, especially when performed from a center with previous experience in double-port VATS approach.
DISCUSSION:Recent advances in surgical and video-assisted techniques have allowed minimally invasive pneumonectomy to be undertaken safely. VATS pneumonectomy is not a new procedure and in fact was initially reported 15 years ago and was felt to result in less postoperative pain and a faster return to normal activities [1]. Despite this, there have been only a few case reports or series published of VATS pneumonectomies [2,3].
Additional References/ Resources
Gonzalez – Rivas, D., Fernandez, R., De la Torre, M., & Martin – Ucar, A. E. (2012). Thoracoscopic lobectomy through a single incision.Multimedia manual cardio-thoracic surgery, Volume 2012. This is an excellent article which gives a detailed description, and overview of the techniques used in single incision surgery. Contains illustrations, full color photos and videos of the procedure.
Gonzalez-Rivas D, Paradela M, Fieira E, Velasco C. (2012). Single-incision video-assisted thoracoscopic lobectomy: initial results. J Thorac Cardiovasc Surg. 2012 Mar;143(3):745-7.