Monaldi Hospital – If these walls could talk

It’s the second day of the conference at Monaldi Hospital which is located in Zona Ospedale, in the hills of Naples. The corridors of the 800 bed, 135 year-old former tuberculosis sanitarium give away few hints of the rich and interesting history of this institution. Commandeered by the Allies during the second world war, and containing a small but extensive pathology museum hidden in a back office, showcasing lung disease and many of the disseminated tuberculosis cases that were cared for here, one can only be intrigued by the stories contained within such as the first specimen in the collection, a five month’s gestational fetus (in utero) of a deceased tuberculosis patient.

But we digress. As intriguing as all the tales of thoracic disease past are, we are gathered here today to advance the present and change the future of thoracic surgery here at Monaldi Hospital. As mentioned in a previous post, the surgeons here in the department of thoracic surgery have only recently adopted VATS surgery. Now after four years of practice, it is time to perfect it. For that reason, the first guest surgeon to perform the live demonstration today is Dr. Henrik Hansen.
Live Surgery with Drs. Hansen & Gonzalez Rivas
Dr. Henrik Hansen

Dr. Hansen is a Denmark native who currently operates in one of Europe’s busiest VATS programs, located in Copenhagen. 80% of all the thoracic surgeries performed at his institution, Rigshospitalet. (In comparison, in most of Europe, VATS comprises of 52% of thoracic procedures, according to data presented by Dr. Hansen).
As the head of the minimally invasive surgery department at Righospitalet, he has mastered and streamlined the ‘traditional’ or three-port VATS approach, so there are no wasted efforts to maximize efficiency.
During a short lecture prior to surgery, Dr. Hansen discussed the literature, including a paper by WS Walker et al. in 2003, which compared cancer survival outcomes in patients undergoing VATS and standard open procedures. In the paper, the authors unequivocally recommended VATS as the operation of choice. It was this paper that led Dr. Hansen to aggressively pursue VATS for the majority of his patients. This position was not echoed in the official guidelines until 2013.
Dr. Hansen allows that not all cases should be VATS cases; he prefers to perform sleeve resections via thoracotomies instead of VATS pneumonectomies, to prevent excess tissue loss in these cases).
Interestingly enough, residents in Dr. Hansen’s program learn VATS techniques without knowing the equivalent open surgical technique. He cites one of his thoracic surgery fellows as performing over 80 VATS procedures but only two thoracotomies. As a surgery purist, this disturbs me in some way, but then again – by much of Dr. Hansen’s criteria, I would be labeled a traditionalist.
For the morning’s case, he is performing a left upper lobectomy. (There are no other case details available to spectators in the auditorium)*.
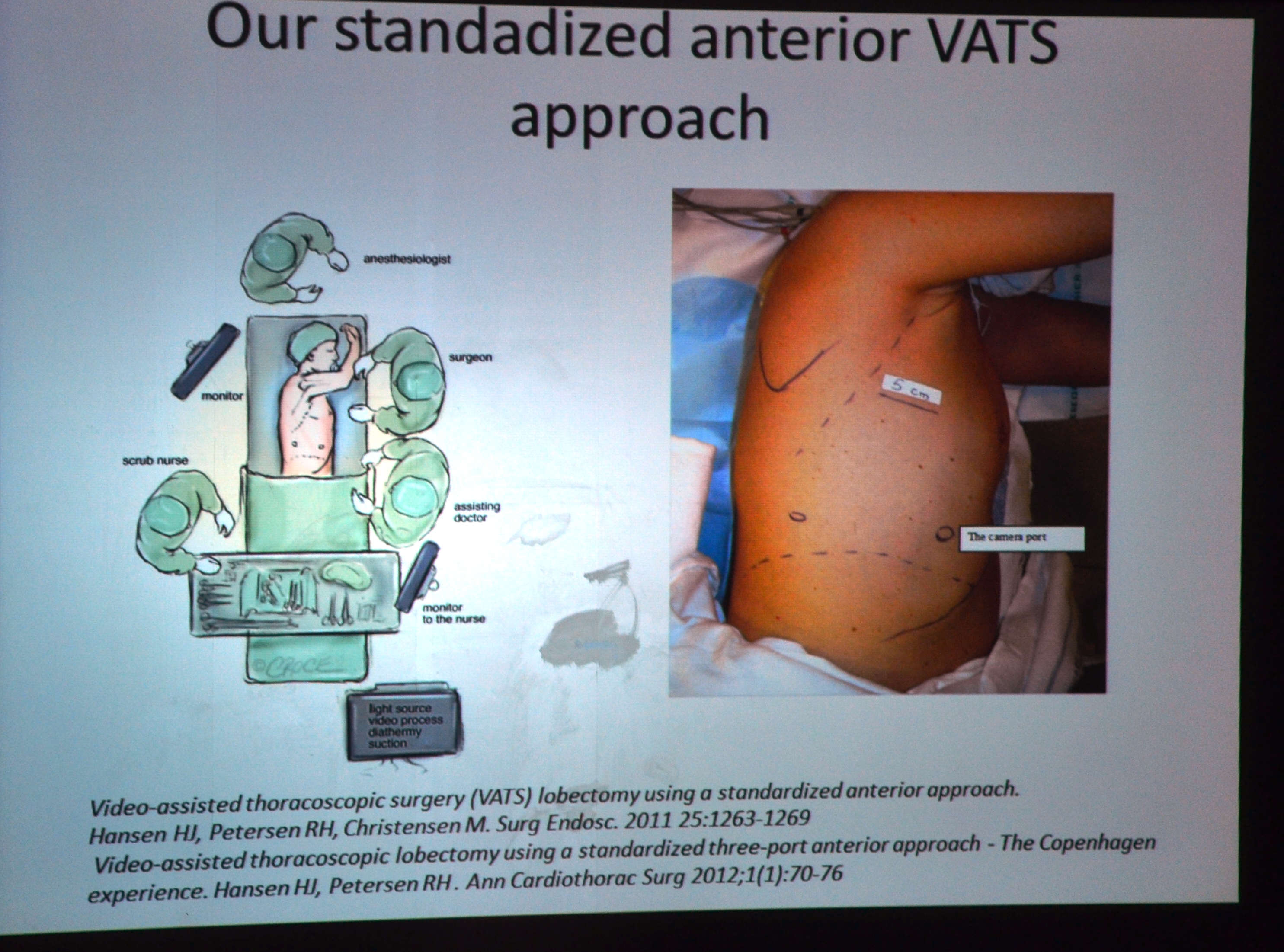
He places the first port along the transverse line where the standard thoracotomy incision would normally be placed. He then triangulates the second and third ports, though only one actual trocar port is used, a 12 mm port for the camera insertion.
The “working” incision is the uppermost incision, which appears to be quite large, (but this may be a distortion due to my perspective – from a camera placed above the operating room table). At times he uses more than one instrument in this incision – and watching him, he seems that he could easily convert to single port surgery with equal efficiency. He almost forgets about his second port at times, and uses the remainder (3rd port) solely for the camera access.
He is precise and exacting in his movements, which is what makes his reliance on traditional VATS a little puzzling. Habit, mainly, I suspect because the surgery proceeds as if by rote. He really is the master of efficiency – and the case progresses quickly.
He uses ligasure for greater precision during dissection and isolation of tissue and minimizes the external torsion and retraction placed on the lung during hilar dissection, isolation and ligation of the pulmonary vasculature. He completes the procedure by performing an extensive lymph node dissection.
*Since I was outside of the operating room for this case, there are not very many operative photos, and none of Dr. Hansen operating.
Dr. Diego Gonzalez Rivas

As part of his pre-surgical lecture, “Recent advances in uniportal VATs,” Dr. Gonzalez reviewed the recent history of uniportal VATS as well as surgical tips for surgeons learning the technique. He also reviewed some of his more recent forays into surgery including complete uniportal resections using only the harmonic scalpel, and surgery on non-intubated (and awake) patients on nasal cannula. He discussed that the non-intubated project was a anesthesia counterpart to minimally invasive surgery. Since the risks and complications related to thoracotomies and other large incisions have been eliminated, it’s a normal progress to advance towards less invasive anesthetic techniques (since general anesthesia is associated with serious risks such as severe hypotension, peri-operative myocardial infarction and cardiovascular collapse). While rare, eliminating general anesthesia in many cases, greatly reduces the risk of adverse anesthesia-related events.
Surgical procedure**: Left upper lobectomy with radial lymph node dissection for a left upper lobe peripheral nodule in a 65 year patient.

Surgeon: D. Gonzalez Rivas. Assistant Surgeon: D. Amore Scrub nurse: Guiseppe

Initial post-intubation vital signs: HR 83, NSR B/P 90/60 Saturation 99%
1445: Initiation of patient prep (betadine). Patient is in a side-lying position.
1510 First incision (only incision)
1515: camera inserted, initial chest cavity inspection, lung deflated. No significant adhesions or unexpected findings. Hilar dissection commences, with attention being given first to the pulmonary artery. By 1605, the left upper lobe branch of the pulmonary artery has been divided.

1608: Bronchus stapled (resected). Patient noted to have an incomplete fissure of the upper lobe.
By 1612: The lobe is out. Dr. Gonzalez proceeds with radical lymph node dissection – including the nodes of the paratracheal area/ aortapulmonary window. The surgical field is essentially dry, with small amount of liquified fat from electrocautery dissection with just minor oozing from the aortopulmonary window. He places a small amount of surgicell in the subcarinal space, after harvesting several nodes to show the best angle of approach (posterior).

During surgery, he spends a few minutes demonstrating alternative techniques to hold and manipulate several instruments in one hand so that surgeons can minimize wasted movements.
After final inspection, Dr. Dario Amore assumes the role of primary surgeon – to place the chest tube (1653). Lung is re-inflated, and the ventilator/ respiratory loop is used to determine that there is no air leak. Camera out of the chest at 1655.
Vital signs: HR 76, NSR B/P 121/62 Sats 100% No hemodynamic instability or hypotension during the case. EBL for the case is around 90ml (+/- 10 ml due to lack of graduations on the suction canister).
Skin incision closed: 1710
By 1715: Patient is awake, extubated and able to verbal respond to commands/ questions.
**Since I was present in the operating room, I was privy to a great deal more information than audience members in the auditorium such as the pre-surgical patient review, monitor readings, etc.
