Dr. Chen and his colleagues at Mackay Memorial Hospital in Taiwan published a new article on their experiences using single and dual port thoracoscopy for diaphragm plication.
The report follows 21 cases from July of 2008 to December of 2011. All 21 cases with left-sided eventrations. 11 were plicated using dual port thoracoscopy in the time period prior to January 2010. In January of 2010, single port thoracoscopy became routine practice at Mackay Memorial. The 10 subsequent cases were all performed by single-port thoracoscopy.
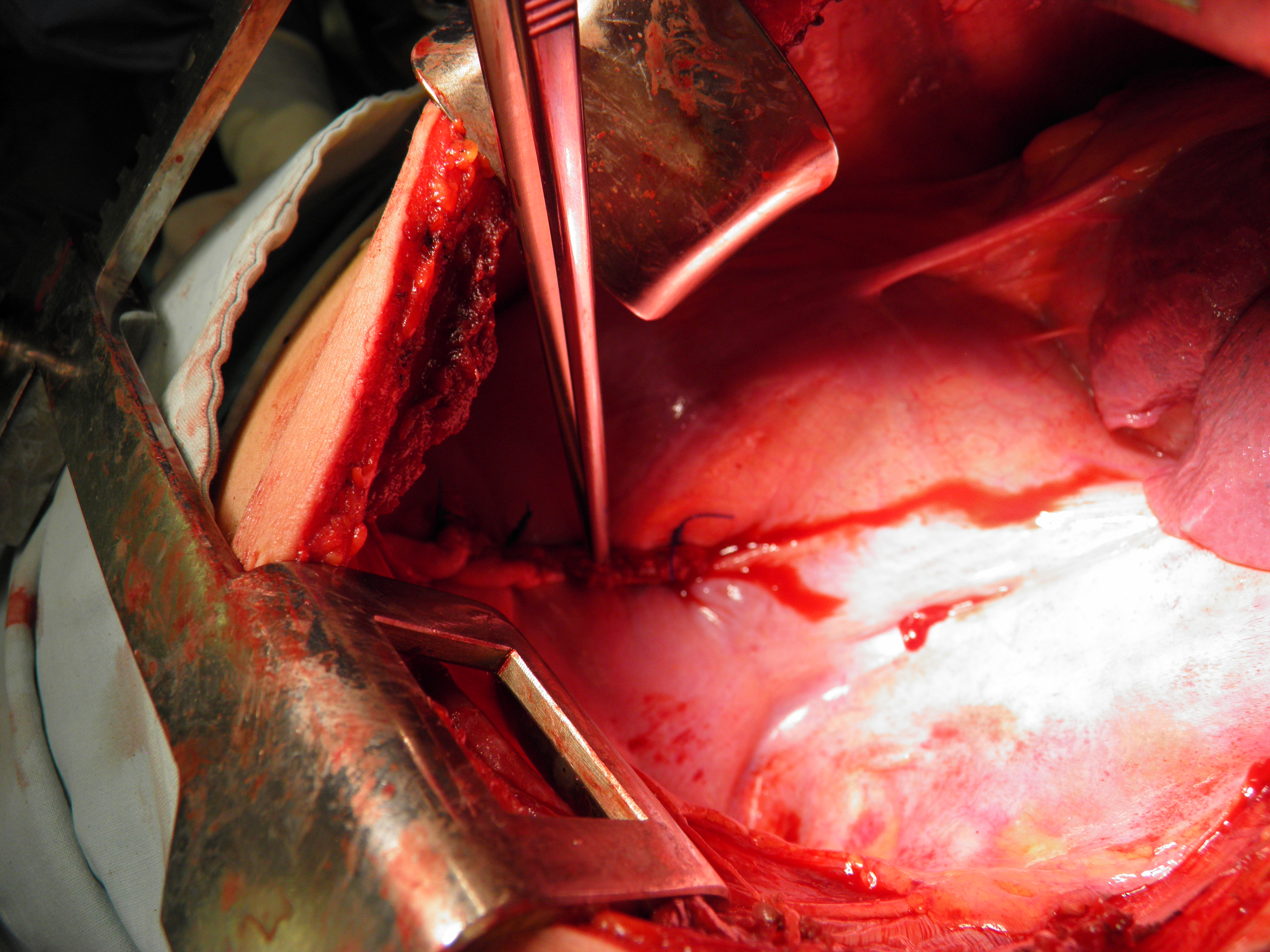
Surgical procedure: The average surgical time between dual port and single port varied by ten minutes with dual port surgery taking longer, averaging 92 minutes. ( see Table 1 of original article). 2.0 silk suture was used for plication of the diaphragm.
Port placement:
In cases using dual port thoracoscopy, the surgeons made the first port at the 7th ICS near the MCL with a second port at the 4th or 5th ICS along the anterior axillary line.
For single port cases, the sole port was 1.5 to 2.0 cm in length and was placed at the 6th ICS along the anterior axillary line.
At the conclusion of the VATS procedure for all patients, a single 24fr or 28fr chest tube was placed, and marcaine was administered as a intercostal block. Patients were extubated prior to leaving the operating room.
The chest tube was removed on the first or second post-operative day. Patients were discharged home following chest tube removal. Post-operative pain scores were minimal, and there was no operative mortality.
The authors discuss surgical technique, and port location for a significant portion of the article. Interested readers are advised to read the original for more details.
Discussion:
Interestingly, while much of the literature on diaphragmatic eventration focuses on early repairs of this condition (neonates and pediatric cases), all of the patients in this series were adults, with an average age of 54 – 55 years of age. Both genders were represented; 15 women and 6 men, with an almost equal distribution among single and dual port cases. (3 men in each group, 7 women in single port, 8 in dual port.)
Unlike traumatic diaphragmatic tear or rupture, diaphragmatic eventration is usually a congenital condition and may be asymptomatic. It is often discovered incidentally after patients undergo radiographic studies for other conditions. However, this condition may predispose patients to other conditions such as respiratory distress or dyspnea by compromising respiratory function on the affected side. In fact, the affected lung may appear tiny, and underdeveloped at the time of repair.
In Dr. Wu and Dr. Chen’s study, patients who underwent dual or single port thoracoscopy reported pain scores of four or less at 24 and 36 hours post-operatively. Post-operative hospitalization was short, with patients being discharged on the first or second post-operative day, with no recurrences or mortality.
Reference Article:
Hsin-Hung Wu, Chih-Hao Chen, Ho Chang, Hung-Chang Liu, Tzu-Ti Hung and Shih-Yi Lee (2013). A preliminary report on the feasibility of single-port thoracoscopic surgery for diaphragm plication in the treatment of diaphragm eventration. Journal of Cardiothoracic Surgery 2013, 8:224. Provisional pdf of free full text article, with radiographs, color photographs.
Resources for Additional Information
Eventration of the diaphragm at Learning Radiology
A. P. Kansal, Vishal Chopra, A. S. Chahal, Charanpreet S. Grover, Harpreet Singh, and Saurabh Kansal (2009). Right-sided diaphragmatic eventration: A rare entity. Lung India. 2009 Apr-Jun; 26(2): 48–50.
Radhiana M Y H, Mubarak MY. (2011). A case of focal eventration of left hemidiaphragm with transthoracic left kidney confused with a traumatic diaphragmatic hernia. Med J Malaysia. 2011 Mar;66(1):60-1. Case report.
Visouli AN, Mpakas A, Zarogoulidis P, Machairiotis N, Stylianaki A, Katsikogiannis N, Tsakiridis K, Courcoutsakis N, Zarogoulidis K. (2012). Video assisted thoracoscopic plication of the left hemidiaphragm in symptomatic eventration in adulthood. J Thorac Dis. 2012 Nov;4(Suppl 1):6-16. Three port VATS in an adult.
